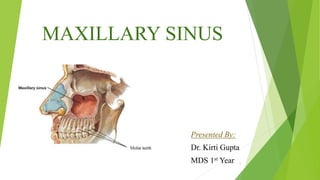
3. INTRODUCTION:
Paranasal sinuses are air filled spaces
present within some bones around the
nasal cavities.
Frontal Sinus
Ethmoidal Sinus
Sphenoidal Sinus
Maxillary Sinus
3
4. Maxillary Sinus is one of the 4 Paranasal Sinuses.
Maxillary sinus is the pneumatic space that is lodged inside the
body of maxilla and that communicates with the environment by
way of the middle meatus and nasal vestibule.
It is a pyramidal shaped concavity.
Anatomy of the Maxillary Sinus was first described by Highmore
in 1651, so also known as Antrum of Highmore.
4
5. DEVELOPMENT:
It is the first Nasal Sinus to develop.
It begins to develop before birth along with sphenoidal sinus.
It starts as a shallow groove on the medial surface of maxilla during the 4th
month of intrauterine life.
It appears as diverticula from the nasal cavity.
The diverticula gradually invades the maxillary bone and therefore is known
as Maxillary Sinus.
5
6. Enlargement of the sinus is associated with overall enlargement of facial
skeleton, including jaws.
Primary Pneumatization of the maxillary sinus occurs at about 3 months of
fetal development by an out-pouching of the nasal mucosa.
Prenatally, a secondary pneumatization occurs.
At birth, the sinuses are filled with fluid.
6
7. Postnatally and until 3 years of age, the growth depends on pressure
exerted by the eye on the orbit floor, tension of superficial musculature
on maxilla and the forming dentition.
At 12 years of age, pneumatization extends to the plane of lateral orbital
wall, and sinus floor is level with the floor of the nose.
The main development occurs as the permanent dentition erupts.
7
9. ANATOMY:
It is the largest Paranasal Sinus.
Communicates with other sinuses through lateral Nasal Wall.
Shape- Pyramidal
Average Dimensions-
Height- 36-45 mm
Width- 23-25 mm
Length- 38-45 mm ( Anterio-posterior Axis )
Average Volume- 15 mL (9.5-20mL)
9
10. Boundaries:
Anterior Wall- Extends from Inferior Orbital Rim to Maxillary Alveolar Processes.
Superior Wall- Floor of the Orbit (very thin)
Posterior Wall- Seperates Maxillary Sinus and Pterygopalatine Fossa
Medial Wall- Lateral Wall of Nasal Cavity
10
12. 12
Relationship between teeth and maxillary sinus (right side).
Note the root of the first premolar (arrow) is located most
medially.
13. Maxillary Sinus Septa:
First mentioned by Underwood in 1910.
Also known as Underwood’s Septa.
Divided on the Base of Origin as :
Primary Septa-
Formed during maxillary development and tooth
growth.
Secondary Septa-
Acquired during the pneumatization of maxillary sinus
after tooth loss.
13
14. Location :
Majority of the septa are are located between the second premolar and
first molar area.
Origin :
They arise from medial or lateral wall of sinus.
14
15. Presence of number of bony septa varies from individual to
individual.
They divide Maxillary Sinus into several recesses.
They may be curved or straight.
Clinical Importance:
Sinus augmentation is usually complicated by the presence of
septa.
15
16. 16
Appears as radiopaque lines within the sinus.
Represents folds of cortical bone projecting few mm away from
the floor and walls of sinus.
17. 17
Possible variations of maxillary sinus septa. 1.Multiple septa , 2.
Single septum , 3.Two septa , 4.Complete septum, 5.Partial horizontal
septum.
18. OSTIUM
Opening of the maxillary sinus is called ostium.
It opens in middle meatus at the lower part of the hiatus
semilunaris.
Lies above the level of nasal floor.
The ostium lies approximately 2/3rd level up the medial wall of
the sinus, making drainage of the sinus inherently difficult.
18
19. 19
Ostium on the left maxillary sinus (arrows). (A) Cadaveric
dissection (anterolateral view). (B) Computed tomography
(coronal image). N, nasal cavity; O, orbit.
20. HISTOLOGY:
Epithelium is pseudostratified, ciliated and columnar.
Maxillary sinus is lined by 3 layers :
Epithelial layer
Basal lamina
Sub epithelial layer with Periosteum
Epithelium, connective tissue and periosteum are collectively called as
Schneiderian Membrane
20
21. Schneiderian Membrane:
Membrane is a pseudostratified columnar respiratory membrane.
Ciliated epithelium formed by the basal cells, columnar cells, and goblet
cells fixed to the basal membrane.
No. of cilia- 100–150 cilia present on each columnar cell
21
22. Vibration of Cilia - at 1000 beats/min
As cilia beats, the mucous on epithelial surface moves from
sinus interior towards nasal cavity.
Thickness of the membrane:
0.13 to 0.5 mm (average 0.8 mm thick)
Importance-
Mesenchymal stem cells from the sinus membrane have an
ability of bone formation, which plays a vital role in sinus floor
elevation procedures.
22
24. Clinical Implications :
Chances of sinus membrane perforation depends on the angle between
the lateral and the medial wall of the sinus i.e.
Greater than 60º angle has 0% chances of perforation.
30º–60º angle has 28.6% chances of perforation.
<30º angle has 62.5% chances of perforation.
Overfilling of the maxillary sinus with the bone graft material may
cause necrosis of the membrane as well as sinusitis and the potential
loss of the bone graft into the sinus.
24
25. 25
The membrane should be freed totally from the caudal area to enable lifting of
the sinus.
26. ARTERIAL SUPPLY :
Greater Palantine Arteries
Infraorbital Artery
Superior Anterior, Middle and Posterior alveolar arteries
26
27. NERVE SUPPLY:
Posterior Superior Alveolar Nerve from Maxillary Nerve
Anterior Superior Alveolar Nerve
Infraorbital Nerve
Middle Superior Alveolar Nerve
Infraorbital Nerve
27
29. FUNCTIONS:
Lightening the weight of the skull.
Humidification and warming of inspired air.
Assisting in regulating intranasal pressure.
Lightening the skull to maintain proper head balance.
Imparting resonance to the voice.
Absorption of shocks to the head.
Filtration of the inspired air.
29
30. CLINICAL EXAMINATION:
INSPECTION :
Middle third of the face should be inspected for the presence of
asymmetry, deformity, swelling, erythema , ecchymosis or hematoma.
EXTRAORAL PALPATION :
Include palpation of the facial wall of the sinus above the premolar where
the bone is thinnest.
30
31. 31
INTRAORAL EXAMINATION:
Examination should be performed for tenderness, or paresthesia of upper
molar and premolar region.
TRANSILLUMINATION TEST:
It is performed in a darkened room by inserting an electrically
safe light into the mouth ( with the lip closed).
Good transillumination indicates presence of air in the sinus while the
failure of transillumination indicates presence of pus, fluid , solid lesion or
mucosal thickening.
32. 32
RADIOGRAPHIC EXAMINATION:
Radiography is the most important supplementary investigation to clinical
examination of the sinuses.
RadiographicMethods
Intra Oral
Extra Oral
Others
34. 34
PERIAPICAL ( IOPA )
The roots of maxillary molars usually lies in close to the
maxillary sinus and may project into the floor of the sinus,
causing small elevations or prominences.
(White & Pharoah 2000)
36. 36
Computerized tomography (CT) & Magnetic Resonance
Imaging (MRI)
These modalities provide multiple sections through the sinuses at
different planes and therefore contribute to the final diagnosis and the
determination of extent of the disease.
CT SCAN MRI
37. 37
ADVANCED METHODS:
Ultrasound
It offers a fast ,reliable and radiation free method for
diagnosing sinusitis.
Ultrasound beam sent out by the sinus ultra is reflected from the posterior
wall of the sinus when the sinus contains fluid and from the anterior wall
when sinus contains air.
38. 38
Diagnostic Endoscopy
It is an optimal method especially for the assessment of foreign bodies
(such as root filling materials and root tips) that have penetrated into the
maxillary sinus.
(Kennedy et al. 1985)
41. Maxillary Sinusitis
Acute Maxillary Sinusitis
Sudden onset
Duration of 4 weeks or less
Subacute Maxillary Sinusitis
Duration of 4–12 weeks
Chronic Maxillary Sinusitis
Duration of atleast 12 weeks
41
42. 42
INFECTIOUS CAUSES
1. Bacterial
2. Viral
3. Fungal
NON INFECTIOUS CAUSES
1. Allergic
2. Non Allergic
3. Pharmacologic
4. Irritants
DISRUPTION OF MUCOCILIARY MEMBRANE
1. Surgery
2. Trauma
ETIOLOGY:
43. Oro-Antral Communication and Oro-
Antral Fistula
Maxillary sinus perforation occurs occasionally during the extraction of
a maxillary tooth, and it may be a cause of maxillary sinusitis or oro-
antral fistula.
The chances of creating an oro-antral fistula in patient less than 15 yrs
are comparatively lesser than in adults due to incomplete development
of sinus.
The distance between apical end of maxillary posterior teeth and floor of
sinus is approximately 1-1.2 cm.
43
45. Maxillary Sinus Pneumatization
The expansion of the sinus is larger, following extraction of several adjacent
posterior teeth.
If dental implant placement is planned in these cases, immediate
implantation and/or immediate bone grafting should be considered to assist
in preserving the 3-dimensional bony architecture of the sinus floor at the
extraction site.
45
46. Implant related Sinus Augmentation
Indications
No history of sinus pathosis.
Insufficient residual bone height (less than 10 mm of bone height).
Severely atrophic maxilla.
Poor bone quality and quantity in the posterior maxilla.
46
47. Contra- indications
Acute active sinus infection
Recurrent chronic sinusitis
Severe allergic rhinitis
Neoplasm or large cyst of the sinus
Previous sinus surgery
History of radiation therapy to maxilla
Presence of Underwood’s septa
Uncontrolled diabetes mellitus
Alcoholic and heavy smoker 47
48. Various techniques for sinus augmentation
Direct/lateral window technique
In this technique, sinus membrane is directly visualized and
instrumented through the window created in the lateral wall of
maxillary sinus.
48
49. Indirect/osteotome technique/crestal approach/transalveolar
approach
• Transalveolar technique was first performed by Tatum.
• Summers later described another crestal approach, using tapered
osteotomes with increasing diameters.
• Indirect osteotome maxillary sinus floor elevation is generally
indicated where the residual bone height is equal to or >6 mm.
49
50. AGE CHANGES :
Sinuses are rudimentary or even absent at birth.
They enlarge rapidly during the ages of 6 to 7 years i.e. at the time of
eruption of permanent teeth and then after puberty.
In old age, the growth is due to resorption of the surrounding bone –
Extension of sinus till the crest.
In the edentulous maxilla, the sinus expands in both inferior and lateral
dimensions and may invade the canine eminence region.
50
51. CONCLUSION:
Due to close proximity of maxillary sinus to orbit, alveolar ridge,
maxillary teeth, diseases involving these structures may produce
confusing symptoms. Hence a precise information about the surgical
anatomy is essential to the surgeons.
Knowledge of the anatomical relationship between the maxillary
sinus floor and the maxillary posterior teeth is important for the
preoperative treatment planning of Maxillary posterior teeth.
Clinicians must be particularly cautious while performing dental
procedures involving the maxillary posterior teeth.
51
52. REFERENCES:
Textbook of General Anatomy, B.D. Chaurasia, 6th Edition.
Textbook of oral and MaxillofacialSurgery, Neelima Malik.
Textbook of oral and MaxillofacialSurgery, SM Balaji.
Textbook of Oral Radiology, Ghoms, 2nd Edition.
Orban’s, Oral Histology and Embryology, 11th Edition.
Clinical Periodontology and Implant Dentistry, Lindhe, 5th Edition.
Contemporary Implant Dentistry, Carl E. Misch, 3rd Edition.
Bathla SC, Fry RR, Majumdar K. Maxillary sinus augmentation. J
Indian Soc Periodontol 2018;22:468-73.
52
53. Kim MJ, Jung UW, Kim CS, et al. Maxillary sinus septa: prevalence,
height, location and morphology. A reformatted computed
tomography scan analysis. J Periodontol 2006; 5:903–908.
Iwanaga, Joe et al. “Clinical anatomy of the maxillary sinus:
application to sinus floor augmentation.” Anatomy & cell biology vol.
52,1 (2019): 17-24. doi:10.5115/acb.2019.52.1.17
Maestre-Ferrín L, Galán-Gil S, Rubio-Serrano M, Peñarrocha-Diago
M, Peñarrocha-Oltra D. Maxillary sinus septa: A systematic review.
Med Oral Patol Oral Cir Bucal. 2010 Mar 1;15 (2):e383-6
Tarun Kumar AB, Anand U. Maxillary sinus augmentation. J Int Clin
Dent Res Organ 2015;7:81-93.
53