

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Pelvic inflammatory diaease
Similar to Pelvic inflammatory diaease (20)
More from Abhilasha verma
More from Abhilasha verma (20)
Recently uploaded
Recently uploaded (20)
Pelvic inflammatory diaease
- 1. PELVIC INFLAMMATORY DIAEASE (PID) PRESENTED BY ABHILASHA VERMA LECTURER (OBG. GYNAE) JHALAWAR NURSING COLLEGE
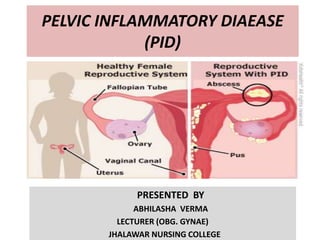
- 2. DEFINITION • Pelvic Inflammatory Disease (PID) is a spectrum of inflammatory disorders of the upper female genital tract, including any combination of endometritis, salpingitis, tubo-ovarian abscess, and pelvic peritonitis.
- 3. ETIOLOGICAL AGENTS • Sexually transmitted organisms, especially N. gonorrhoea and C. trachomatis, are More common. • Microorganisms of the vaginal flora (e.g., anaerobes, G. vaginalis, Haemophilus influenzae, enteric Gram-negative rods, and Streptococcus agalactiae) also have been associated with PID • M. [Mycoplasma] hominis and U. [Ureaplasma] urealyticum might be etiological agents of PID.
- 4. EPIDEMIOLOGY • PID is commonly associated with Sexually Transmitted Diseases (STDs) • About 85% are spontaneous infection in sexually active females of reproductive age. • Iatrogenic procedures: favor organism to ascend 1. Endometrial biopsy 2. Uterine curettage 3. Insertion of IUD 4. Hysterosalpingography
- 5. 34% 66% DISTRIBUTION A/C AGE >25 YEARS <25 YEARS85% 15% EPIDEMIOLOGY STD IATROGENI C 95% 4%1% CLINICAL PRESENTATION ASYMPOTOMATIC MILD TO MODERATE SEVERE
- 6. RISK FACTORS 1. Menstruating teenagers. 2. Multiple sexual partners. 3. Previous history of acute PID. 4. IUD users. 5. Sexual partner with urethritis or STI. 6. Prior infection with chalmydia or gonorrhoea. 7. Younger age of onset of sexual activity. 8. Sexually transmitted infection. 9. Low socio-economic condition. 10. High frequency of sexual intercourse. 11. No use of contraceptive barrier methods. 12. Intercourse during PID.
- 7. PROTECTIVE FACTORS • CONTRACEPTIVE PRACTICES • Barrier method specially condom, diaphragm with spermcide. • Oral steroidal contraceptives , produce thick mucus plug which prevent going up of sperm and bacterial penetration. • Monogamy or partner with vasectomy. • OTHERS • Pregnancy • Menopause • Azoospermic male
- 8. MICROBIOLOGY ACUTE PID: • Usually poly microbial Primary organisms • Sexually transmitted Secondary organisms - Normally found in vagina • Aerobic: Non-hemolytic streptococcus, E. coli, Group-B streptococcus & staphylococcus • Anaerobic: Bacteroides species- fragilis & bivius, Peptostrepococcus & peptococcus 16% 16% 5%63% MICROBIOLOGY N. gonorrhoeae Chlamydia trachomatis Mycoplasma hominis Others
- 9. MODE OF TRANSMISSION ASCENDING INFECTION (CANALICULAR SPREAD)- Ascend of gonococcal & chlamydial organisms by surface extension from the lower genital tract through the cervical canal by way of the endometrium to the fallopian tubes . Facilitated by the sexually transmitted vectors such as sperms & trichomonads Reflux of menstrual blood along with gonococci into the fallopian tubes may be the other possibility.
- 12. THROUGH UTERINE LYMPHATIC & BLOOD VESSELS ACROSS PARAMETRIUM- Mycoplasma hominis Secondary organisms
- 14. GYNECOLOGICAL PROCEDURES FAVORING ASCEND OF INFECTION- E.g. D&C, D&E BLOOD-BORNE TRANSMISSION - Pelvic tuberculosis DIRECT SPREAD FROM CONTAMINATED STRUCTURES IN ABDOMINAL CAVITY- E.g. Appendicitis, cholecystitis
- 15. ACUTE PID PATHOLOGY • Involvement of the fallopian tubes is almost bilateral • Pathological process is initiated primarily in the endosalpinx . • It usually follows menses due to loss of genital defence. • Gross destruction of epithelial cells, cilia & microvilli. • Acute inflammatory reaction: all layers are involved. • Tubes become edematous & hyperemic; exfoliated cells & exudate pour into lumen & agglutinate the mucosal folds. • Abdominal ostium: closed by edema & inflammation Uterine end: closed by congestion.
- 16. • Depending on the virulence: watery or purulent exudate • Hydrosalpinx or Pyosalpinx. • Deeper penetration & more destruction. • Possibilities Oophoritis Tubo-ovarian abscess Peritonitis Pelvic abscess or Resolution in 2-3 weeks with/without chronic sequela • Depending on the virulence: watery or purulent exudate • Hydrosalpinx or Pyosalpinx • Deeper penetration & more destruction • Possibilities Oophoritis Tubo-ovarian abscess, Peritonitis, Pelvic abscess or Resolution in 2-3 weeks with/without chronic sequel.
- 18. CLINICAL FEATURES SYMPTOMS- Patients with acute PID present wide range of non specific symptoms, usually appears at the time and immediately after menstruation. Bilateral lower abdominal & pelvic dull aching pain is characteristic of acute PID. The onset of pain is more rapid in gonococcal infection (3 day) then of chalmydia infection ( 5-7 Days) Nausea, vomiting, lassitude, headache. Fever (Oral temperature > 38.3˚C/101F) Abnormal vaginal discharge becomes purulent and copious. Symptoms suggestive of dysuria. Dyspareunia. Pain and discomfort in right hypochondrium region ( upper), pain resulting from ascending pelvic infection and inflammation of the liver capsule or diaphragm. Liver involved due to transperitoneal or vascular dissemination of either gonococcal or chlamydial infection. ( Fitz-Hugh-Curtis syndrome)
- 19. SIGN • Temperature >38.3° C • Abdominal palpation reveal tenderness on both quadrants of lower abdomen. Liver may be enlarged and tender. • Vaginal examination reveals – 1) Abnormal vaginal discharge , may be purulent. 2) Congested external urethral meatus or opening of bartholine’s ducts through which pus may be seen scraping out on pressure. 3) Speculum examination reveals congested cervix with purulent discharge. 4) Bimaual examination reveals bilateral tenderness on fornix palpation, which increases more with movement of cervix ( Cervical motion tenderness) also known as (Chandelier sign) Thickening or a definite mass felt through fornices.
- 20. Definitive criteria •Histopathologic evidence of endometritis on bipsy. •Imaging study TVS/MRI evidence of thick fluid filled tubes , tubo ovarian abscess. •Laparoscopic evidence of PID
- 21. INVESTIGATIONS • Complete blood count • Erythrocyte sedimentation rate • Vaginal wet mount 1. WBCs suggest PID 2. Genetic probe or culture of vaginal secretions for gonorrhea and chlamydia 3. Nucleic acid amplification tests (NAATs) for organisms • C – reactive protein • Urine Pregnancy Test (UPT), urinalysis • Urine culture and sensitivity • Urine NAATs • Faecal occult blood test • Tests for tuberculosis • Tests for syphilis • Tests for HIV
- 22. DIFFERENTIAL DIAGNOSIS 1. Appendicitis 2. 2. Ectopic pregnancy 3. 3. Endometritis 4. 4. Ovarian cyst 5. 5. Ovarian torsion
- 23. COMPLICATION OF PID IMMEDIATE • Pelvic perotinitis • Generalised perotinitis. • Septicemia producing arthritis, myocarditis. LATE • Dyspareunia • Infertility 12%, after two episode 25%, after three episode 50%. Due to tubo- ovarian mass. • Chronic pelvic inflammation • Formations of adhesions • Hydrosalpinx • Tubo-ovarian abscess. • Increase risk of ectopic pregnancy.
- 24. TREATMENT ESSENTIAL STEPS- • Public health awareness. • Prevention of STDs • Health education regarding safer sex practices. • Use of contraceptives. • Routine risk of high risk population. PRINCIPLES OF THERAPY- • To control infection • To prevent complications. • To prevent re-infection.
- 25. OUT PATIENT THERAPY- • Adequate rest & analgesics. • Antibiotics even before microbial report. • Combination antibiotics given. • Ceftrixone 250mg IM single dose • Doxycycline 100 mg bid for 14 days with or without • Metronidazole 500mg bid 14 days. • Evaluated after 48 hrs and if no response, are to behospitalised. IN PATIENT THERAPY- • Hospitalization. IV fluids only – Suspected tubo-ovarian abscess – Surgical emergencies. – Unresponsive out-patient treatment. – Intolerance to oral abs. – Co-existing pregnancy. – Patient is known to have HIV infection. Regimen A Cefoxitine 2 gm IV 6 hrly for 2-4 days + doxycycline 100 mg bid for 14 days. Regimen B Clindamycin 900 mg IV 8 hrly + gentamycin 2 mg/kg IV ( Loading) follwed by 1.5 mg/kg IV ( maintenance) every 8 hrly. Alternative Regimen – Ampicillin- salbactum 3gm IV 6hrly 3-5 days + Doxycycline 100 mg oral bid for 14 days.
- 26. MANAGEMENT PROTOCOL YES NO YES NO YES NO History physical examination & pregnancy test PREGNANCY Cervical motion, uterine and adnexal tenderness. Consider surgical consultation, laparotomy for appendicitis consider USG and abdominal & pelvic CT Evaluate for ectopic pregnancy with β-HCG test and TVS Consider PID, TVS to evaluate tubo- ovarian abscess
- 27. YES NO YES NO Pelvic mass on examination Dysuria and white blood cells on urinanalysis Evaluating UTI or pyelonephritis; obtain urine culture Consider ovarian cyst, ovarian torsion, degenerating uterine fibroid, endometriosis, obtain TVS TVS to evaluate for other diagnosis
- 28. SURGERY INDICATION • Generalized perotinitis. • Pelvic abscess • Tubo-ovarian abscess not responding. • Adhesions .
- 29. RE-INFECTION PREVENTION • Educate about re-infection avoidance need and potential hazards of re-infection. • Warned against multiple sexual partners. • Contraceptive practices. • Seek medical attention at early time period. • Follow up visits as schaduled.
- 30. FOLLOW UP • Repeat smear and culture on 7th day from discharge. • Repeat microbial test following each menstrual period until become negative for three consecutive reports when patient declared cured. • Avoid sexual intercourse until both partners declared cured. • Proof of successful treatment after salpingitis ia an intra uterine pregnancy.