Umbilical cord and cord abnormalities
•
27 likes•18,850 views

like share subscribe my you tube channel.. " Lecturer by Abhilasha Verma" for video explaination

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Umbilical cord and cord abnormalities
Similar to Umbilical cord and cord abnormalities (20)
More from Abhilasha verma
More from Abhilasha verma (20)
Recently uploaded
Recently uploaded (20)
Umbilical cord and cord abnormalities
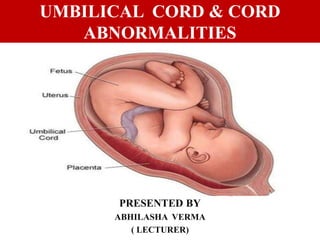
- 1. UMBILICAL CORD & CORD ABNORMALITIES PRESENTED BY ABHILASHA VERMA ( LECTURER)
- 2. STRUCTURE OF UMBILICAL CORD • It is the connecting link between placenta and fetus through which fetal blood flows to and from placenta. • It extends from fetal umbilicus to fetal surface of placenta. • Development: Developed from connecting stalk and body stalk. • Length: 50 – 60 cm • Diameter: 2 cm. (1.5 cm) • Shape: Tortous, showing false notes. • Attachments: It is attached to fetal surface of placenta near its center, the other attachment is to ventral aspect of fetal abdominal wall. • Contents: 2 umbilical arteries, one umbilical vein embedded in wharton’s jelly and surrounded by amniotic membrane.
- 3. • Amnion covers the umbilical cord except near the fetal insertion, where an epithelial covering is substituted. • The arteries wind around the umbilical vein in a spiral fashion and, because the vessels are longer the cord itself, there are a number of foldings or tortuorties producing protusions or false knots on the cord surface. • The Wharton jelly protects the vessels from undue torsion and compression. • Functions: – It contains umbilical vessels that connect the fetus to the placenta. – Allows free movement to fetus
- 4. ABNORMALITIES Abnormal cord Length Abnormal cord diameter Cord Coiling Single Umbilical Artery Four-vessel cord Abnormalities of cord insertion Torsion and Strictures Hematoma Cysts
- 5. Abnormal Cord Length • Normal cord length is 50-60cm, averagely 55cm • Short cord: < 35cm is defined as short cord, (It may lead to fetal distress, placental abruptio, prolonged labour). • Long cord: > 80cm is defined as long cord, higher occurrence of cord around neck, cord around body. (It may leads to true cord knot, cord prolapse and cord compression)
- 6. ABNORMAL CORD LENGTH SHORT CORD LONG CORD
- 7. Umbilical Cord Diameter • Lean cords are associated with IUGR • Large diameter cords are associated with macrosomia
- 8. Umb. Cord Coiling Cord vessels spiral through the cord UCI ( Umbilical Coiling Index ) - is the no. of complete coils divided by the cord length in cm They grouped the UCI as follows: • < 10th percentile — Hypocoiled; • 10th – 90th percentile — Normocoiled; • > 90th percentile — Hypercoiled. Hyper coiling is linked with fetal demise, IUGR & intrapartum hypoxia.
- 11. Abnormalities of U. Cord Insertion • Usually the cord is inserted at or near the center of the fetal surface of placenta. • Various cord insertion variations are: Marginal Insertion ( Battledore Placenta ) Furcate insertion Velamentous insertion Vasa praevia
- 12. Furcate insertion- • Umbilical vessels separate from the cord substance before their insertion into the placenta • Rare Margnial Inserion- • Found in Battledore placenta : cord insertion at the placental margin 7% at term. • Cord being pulled off during delivery of the placenta. Velamentous Insertion – • Umbilical vessels separate in the membranes at a distance from the placental margin ABNORMAL CORD INSERTION
- 15. ABNORMAL CORD INSERTION BATTLEDORE INSERTION VELAMENTOUS INSERTION
- 16. Abnormalities Of Vessels Number Single umbilical artery : Results due to atrophy of the previously existing umbilical artery. • 30% of all infants with only one umbilical artery have congenital anomalies . • Aneuploidies • Tracheo-oesophagial fistula • Renal agenesis • Imperforate anus • Vertebral defects • 34% are growth restricted • 17% deliver preterm
- 18. Knots False knots : • Result from kinking of the vessels to accommodate length of cord and are due to redundancies of Umbilical vessels / Wharton’s jelly.
- 19. True Knots • Incidence 1 – 2 % • More common in monoamniotic twins • Active fetal movements create true knots • Risk of still births is increased 5 to 10 folds in those with true knots. • FHR abnormalities are common during labor but cord blood PH values are normal .
- 20. Umb. Cord Loops The cord is frequently coiled around the fetus More likely with longer cords Loops around fetal neck are termed a nuchal cord. Contractions may compress the nuchal cord and cause FHR decelerations and low umbilical artery Incidence : • 1 loop of Nuchal cord 20-34% • 2 loops of nuchal cord 2.5-5% • 3 loops of nuchal cord 0.2-0.5%
- 21. Two types of cord loops around the fetal neck Type A- Umbilical nuchal cord encircles the fetal neck in a sliding manner (less dangerous). Type B- Nuchal cord encircles the neck in a locking manner (very dangerous). TYPE B
- 22. Torsion & Stricture Torsion : Rare Result from fetal movements during which the cord normally becomes twisted fetal circulation is compromised. Stricture : More serious Most infants with this finding are stillborn Associated with an extreme focal deficiency in Wharton jelly. In mono amnionic twins, a significant fraction of the high perinatal mortality rate is attributed to entwining of the umbilical cords before labor.
- 23. TORSION
- 24. CORD STRICTURE
- 25. Hematoma • Accumulations of blood are associated with short cords, trauma and entanglement. True cysts: Remnants of the allantois. False Cysts: Due to degeneration of wharton’s jelly. • Single cyst may resolve completely • Multiple cysts may be associated with miscarriage /aneuploidy. Umb. Cord Cysts
- 26. THANK YOU