This document discusses abscesses, including:
1. An abscess is a collection of pus surrounded by inflamed tissues and contains dead and dying white blood cells and bacteria.
2. Abscesses spread along paths of least resistance and increase pressure, causing pain. They eventually burst spontaneously or require incision and drainage.
3. Treatment involves rest, elevation, antibiotics, and incision and drainage surgery to fully open and curette the abscess cavity.
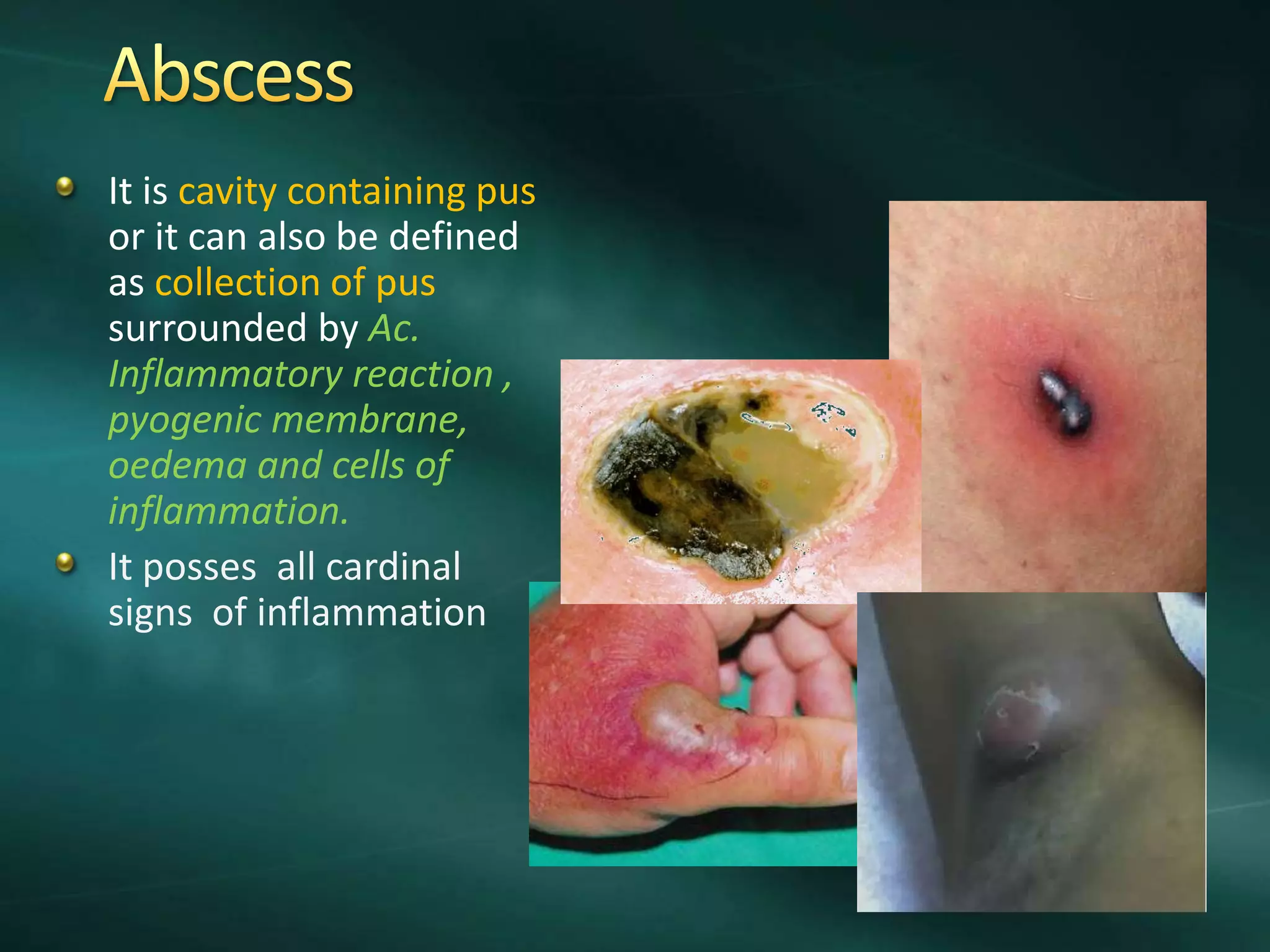
It is cavitycontaining pus
or it can also be defined
as collection of pus
surrounded by Ac.
Inflammatory reaction ,
pyogenic membrane,
oedema and cells of
inflammation.
It posses all cardinal
signs of inflammation
2.
Pus : collectionof dead / dying leucocytes & bacteria
Pyogenic Membrane : An area immediately around the
abscess infiltrated by leucocytes & fibrinous exudate
3.
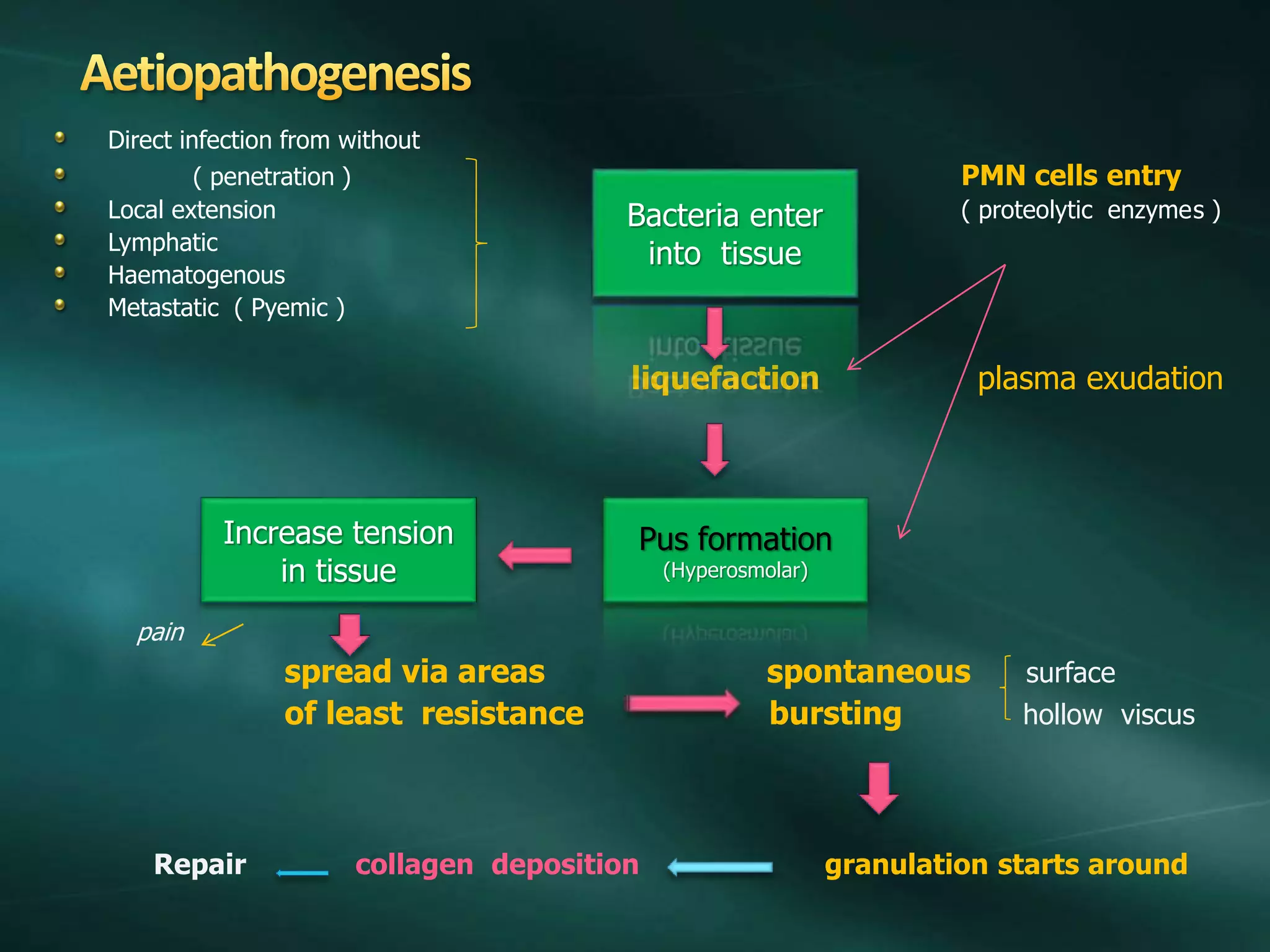
Direct infection fromwithout
( penetration ) PMN cells entry
Local extension ( proteolytic enzymes )
Lymphatic
Haematogenous
Metastatic ( Pyemic )
liquefaction plasma exudation
pain
spread via areas spontaneous surface
of least resistance bursting hollow viscus
Repair collagen deposition granulation starts around
Bacteria enter
into tissue
Pus formation
(Hyperosmolar)
Increase tension
in tissue
4.
pathology
Abscess is surroundedby Acute inflammatory response , pyogenic membrane
( fibrinous exudate ) , oedema and cells of acute inflammation
Pus composed of dead and dying WBC release cytokines , oxygen free
radicals , other molecules
Abscess contains hyperosmolar fluid that draws in fluid. This increases pressure
causing pain .
Spread occurs along the planes of least resistance & point towards skin.
It then burst spontaneously /needs I & D.
Later granulation tissue ( macrophages , fibroblasts, angiogenesis ) forms
around suppurative process --- collagen deposition.
If untreated / resorbed completely - Chronic abscess formation.
In chronic abscess lymphocytes and plasma cells are seen. There is tissue
sequestration and later calcification.
Some organisms are associated with chronicity -- Mycobacteria / actinomycosis
Features
Depends on :size of abscess , virulence of
organism ,tension in the cavity .
Sense of illness
throbbing pain ( increases with dependency )
Pyrexia
Rigors (due to toxaemia / septicaemia )
Local signs of inflammation - calor ,dolor ,rubor ,tumor
loss of function
( due to hyperemia & inflammatory exudate )
7.
Haematological CBC ,ESR
Bio chemical BUN , Sr Creatinine
LFT
Blood sugar
Pathological Swab / scrapings
Radiological X - Ray
USG
CT Scan , MRI
8.
Treatment
Rest
Elevation of affectedpart
Appropriate antibiotics
Surgery – I & D ( Modified Hilton’s Method )
Aspiration ( for liver abscess , retrosternal abscess ,lung abscess )
9.
I & D: points to remember
Before I & D always confirm the diagnosis by appropriate investigations &
always confirm liquefaction of pus .
Drain the abscess by Hilton’s / modified Hilton’s method .
All loculi need to be opened and curetted.
Clean the abscess cavity after I & D and allow it to heal by secondary
intention .
Location of abscess in deep cavities like pleura & peritoneum ( due to
perianastomotic infection or leak ) is difficult to locate . But with the help of
CT /MRI /USG / isotope scan it can be detected and aspirated under guidance
Role of antibiotics is controversial but definitely required if abscess is
spreading.
Surgical drainage & curettage should be adequate whether antibiotics used or
not.
Primary closure can be tried but it is safe to allow healing by secondary
intention.
10.
Spread
Inadequate drainage sinus / fistula
Damage to vital structures
Formation of antibioma e.g. breast abscess
Incision of aneurysm
Formation of chronic abscess.
11.
Abscess needs drainageand curettage .
Modern imaging technique may allow
guided aspiration.
Antibiotics required if abscess is not located
( i.e. cellulitis )
Healing by secondary intention is
encouraged.
12.
Abscess formation dueto spread of infection beyond tonsil
involving tonsiller bed
Quinsy is an old term synonymous with
peritonsillar abscess.
It is derived from the Latin word cynanche
meaning sore throat.
13.
Aetiopathogenesis
PTA usually arisesas a complication of an untreated or partially
treated episode of acute tonsillitis.
The infection, in these cases, spreads to the peritonsillar area
(peritonsillitis). This region comprises loose connective tissue and is
hence susceptible to formation of abscess.
PTA can also occur de novo.
Both aerobic and anaerobic bacteria can be causative. Commonly
involved species include streptococci, staphylococci and hemophilus.
14.
Clinical features
Adults commonlyaffected
Symptoms starts appearing 2-8 days before abscess development
Progressively worsening unilateral sore throat and pain are the earliest
symptoms.
Sudden deterioration with severe pain during attack of tonsillitis
Fever, malaise, headache & distortion of vowels informally known as "hot
potato voice" may appear.
Neck pain associated with tender, swollen lymph nodes, referred ear pain and
halitosis are also common
Increase salivation.
Trismus ( difficulty in opening mouth – due to spasm induced in pterygoid
muscle due to infection )
15.
clinical features
On examination( good illumination and suction may required )
• Erythematous, swollen tonsil with
contralateral uvula displaced medially
• Trismus
• Edema of palatine tonsils
• Diffuse swelling of soft palate
• superior to affected tonsil
Purulent exudate on tonsils
• Drooling
• Muffled, “hot potato” voice
• Cervical lymphadenopathy
• Abscess may point out.
Treatment
Abscess not pointing
Broadspectrum antibiotics.
NSAID
Abscess pointing
I & D required
Adult Children
Local anesthesia Gen anesthesia
2% lignocain spray
Pt sits upward
Incision – midway bet
- ween uvula
& upper 3rd
molar
Forcep pushed & open
Pus drained
19.
complications
Parapharyngeal abscess
Extension ofabscess in other deep neck spaces leading to airway
compromise
Septicaemia
Possible Necrosis of surrounding deep tissues
In rare cases, Mediastinitis