This document discusses hepatitis B, including its transmission, epidemiology, virology, and relationship to liver cancer. Some key points covered are:
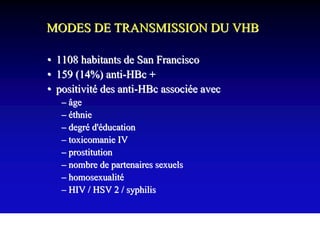
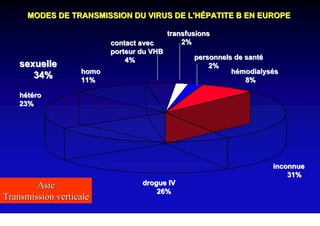
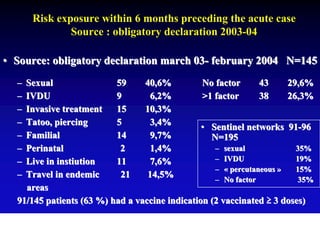
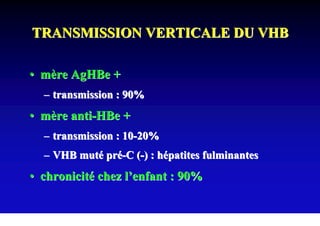
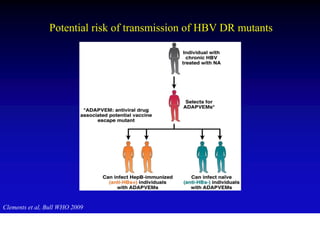
- Hepatitis B virus can be transmitted sexually, through blood exposure or mother-to-child transmission.
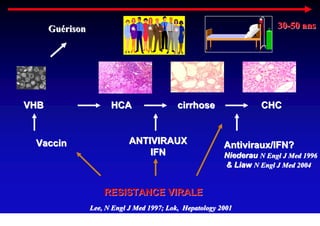
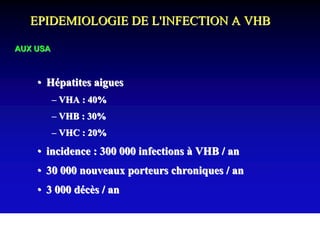
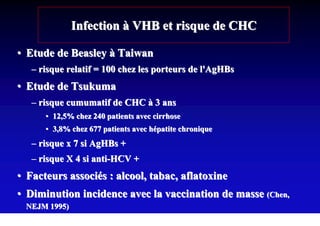
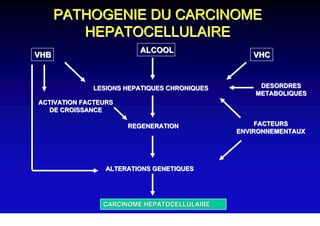
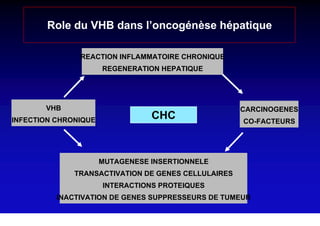
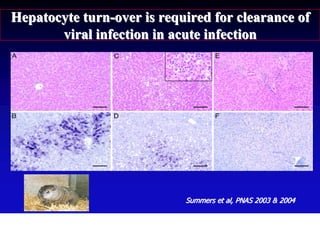
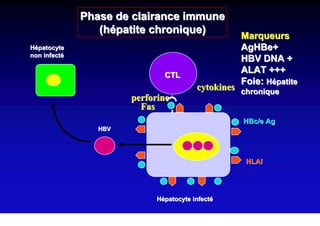
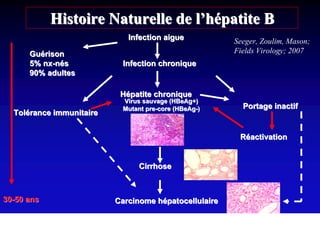
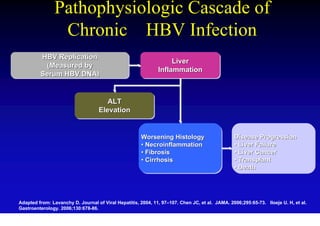
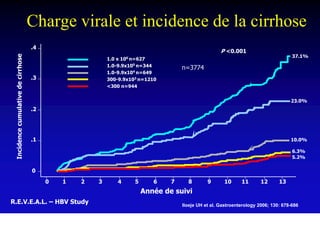
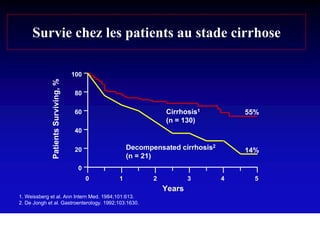
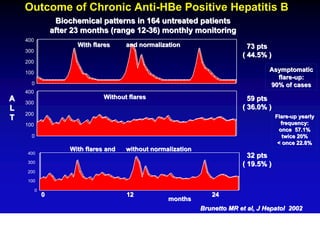
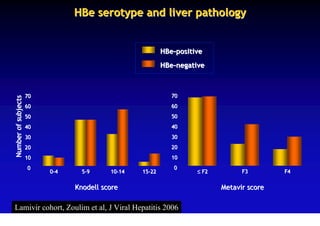
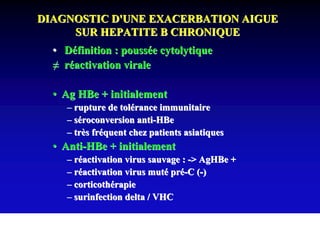
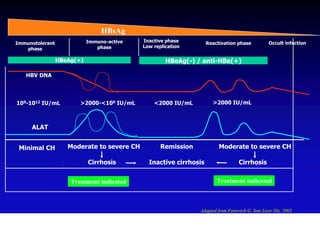
- Chronic hepatitis B infection can lead to cirrhosis and hepatocellular carcinoma over 30-50 years.
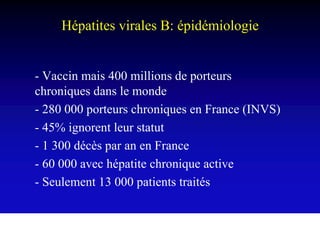
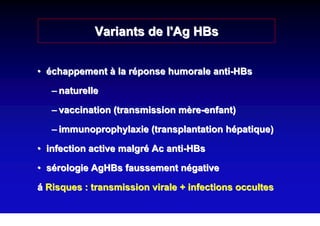
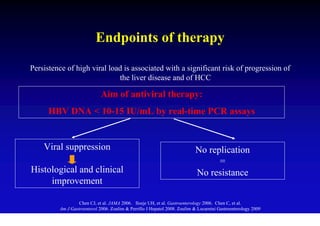
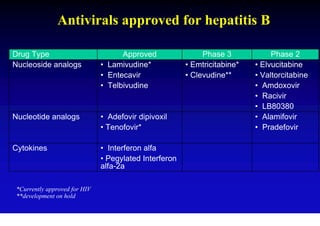
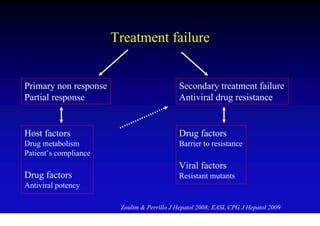
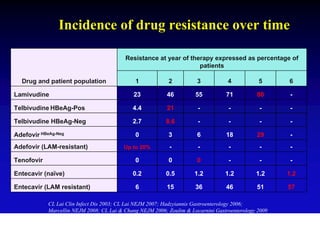
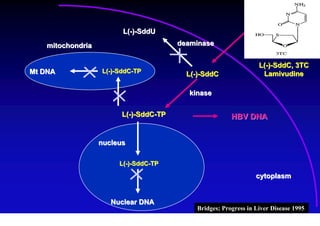
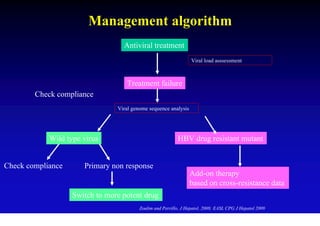
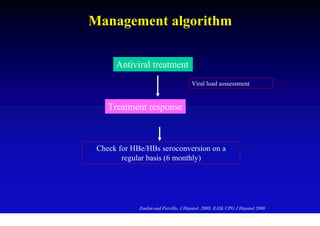
- Antiviral treatments and vaccines have reduced transmission and complications of hepatitis B.
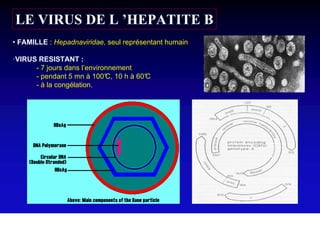
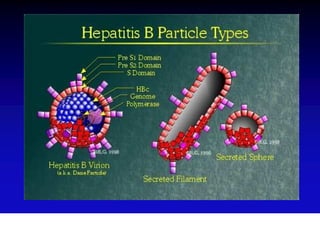
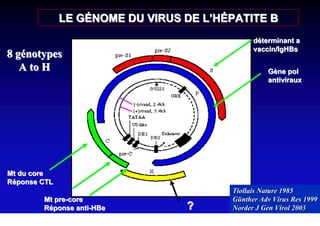
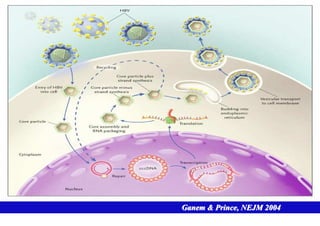
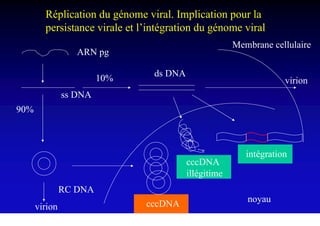
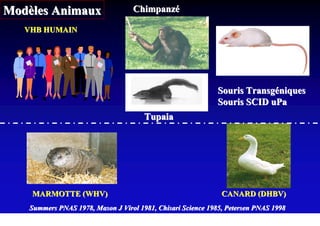
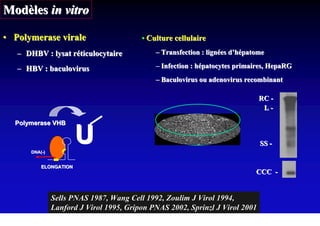
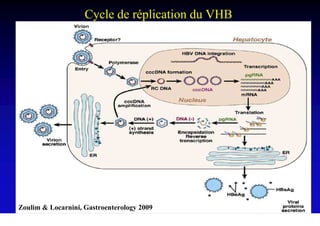
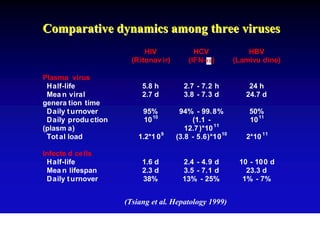
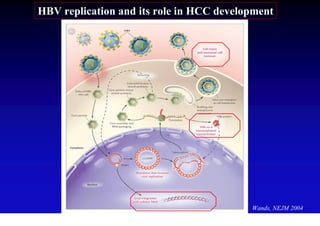
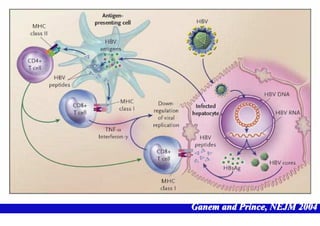
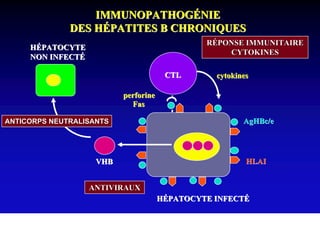
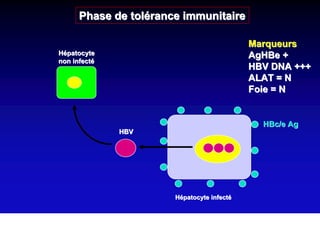
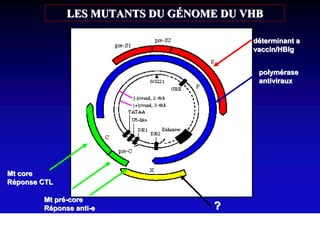
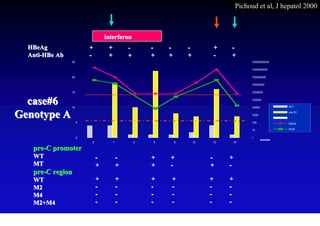
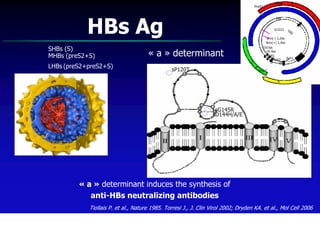
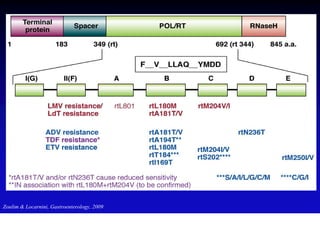
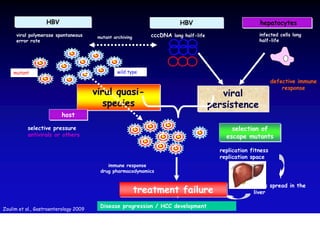
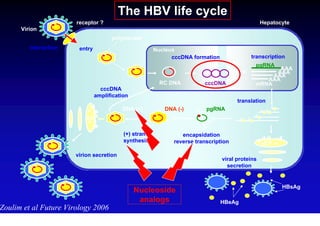
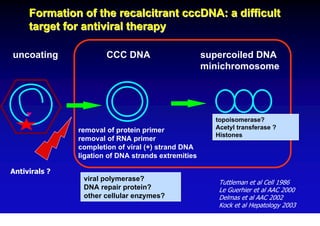
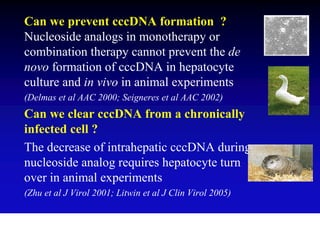
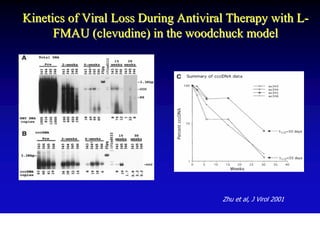
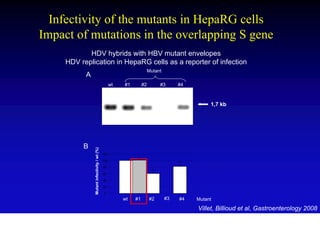
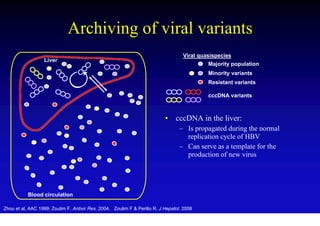
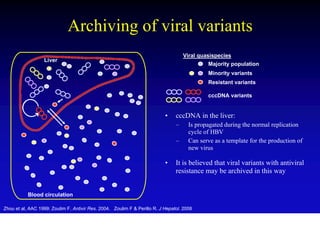
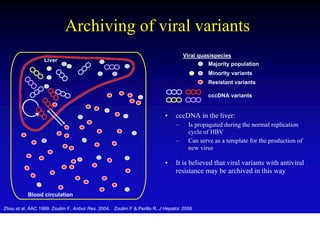
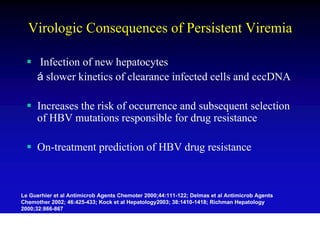
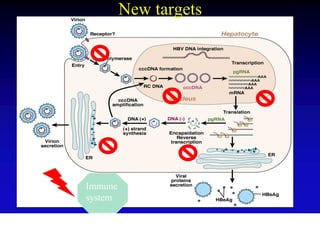
- The hepatitis B virus genome and life cycle allow it to persist chronically in the liver more than other viruses like hepatitis C and HIV.
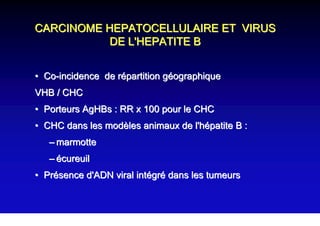
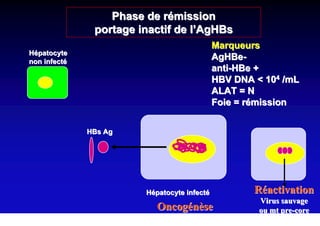
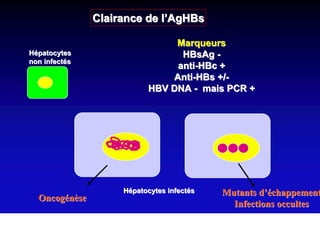
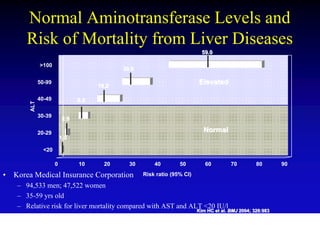
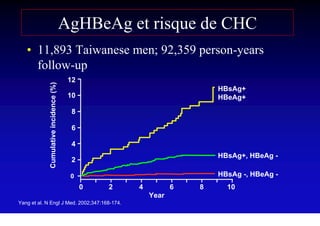
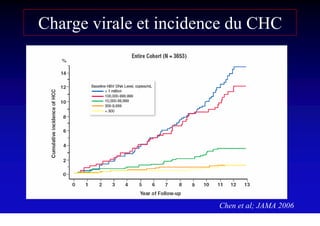
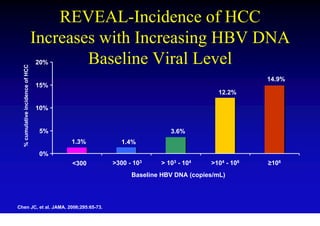
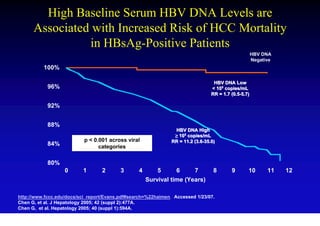
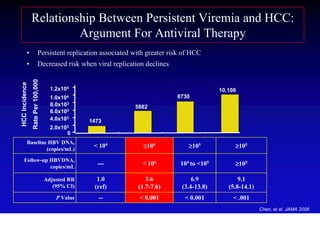
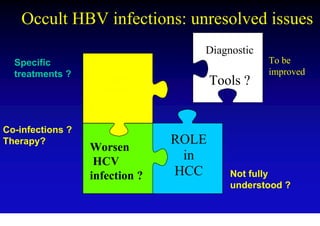
- Chronic hepatitis B is a major risk factor for the development of hepatocellular carcinoma














































![Mediat bibliothèques et droit de l'information [lecture seule] [mode de compa...](https://cdn.slidesharecdn.com/ss_thumbnails/mediatbibliothquesetdroitdelinformationlectureseulemodedecompatibilit-130131072858-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
































































