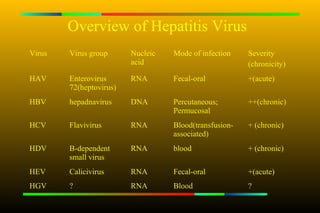
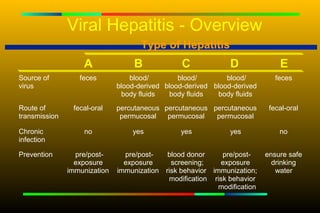
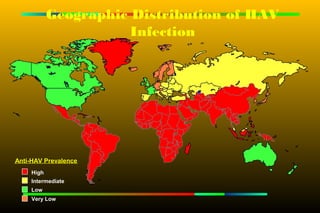
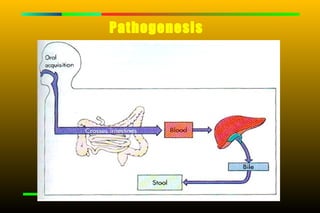
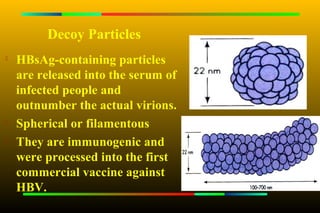
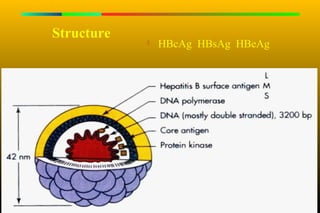
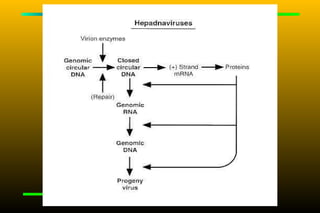
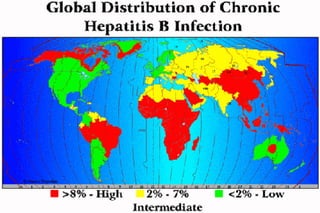
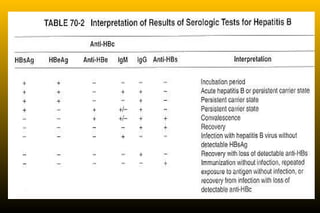
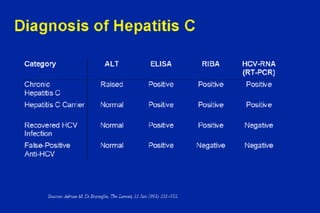
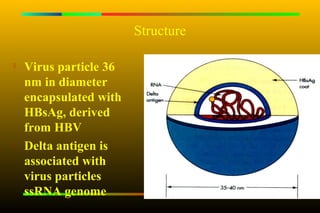
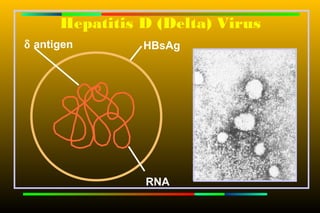
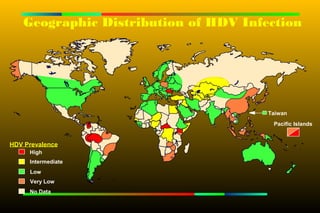
This document summarizes information about Hepatitis virus prepared by Abubakr Sdiq Sargaty. It provides an overview of different Hepatitis viruses including HAV, HBV, HCV, HDV and HEV. Key details include their nucleic acid, mode of transmission, severity and chronicity. The document also discusses viral replication, geographic distribution, clinical features, pathogenesis, diagnosis and treatment of Hepatitis B virus in more depth. It emphasizes the importance of vaccination programs in eliminating HBV transmission.