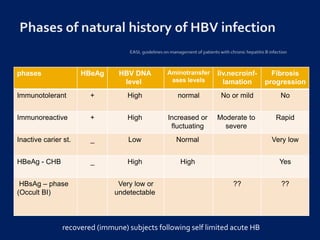
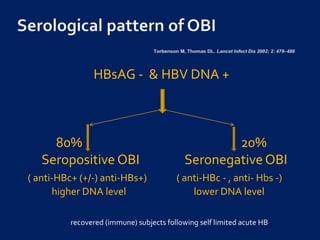
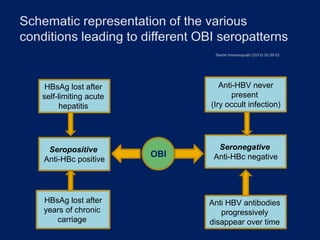
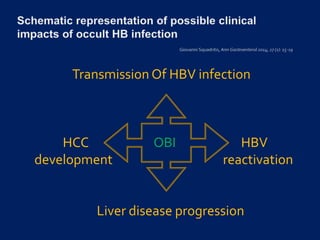
Occult hepatitis B virus infection (OBI) is defined by an undetectable HBsAg but detectable intrahepatic HBV DNA. It can be seropositive (anti-HBc+) or seronegative (anti-HBc-). OBI is characterized by very low or undetectable HBV DNA levels due to strong suppression of viral replication through immune pressure and epigenetic factors. However, OBI can reactivate and cause acute hepatitis. It also poses long-term risks like progression of liver disease to cirrhosis and development of hepatocellular carcinoma through its tumorigenic properties and persistent necroinflammation. Detection requires highly sensitive PCR techniques.









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








