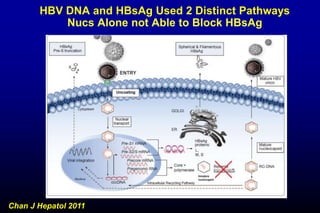
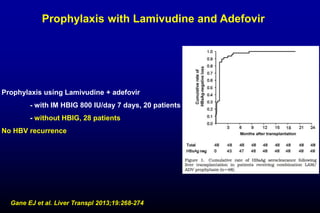
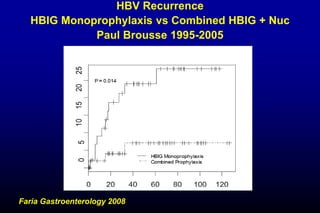
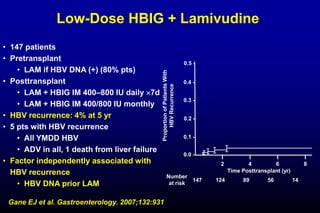
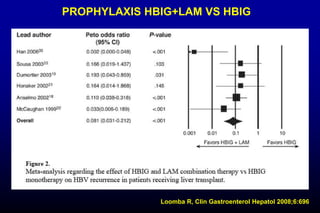
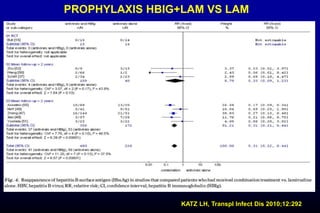
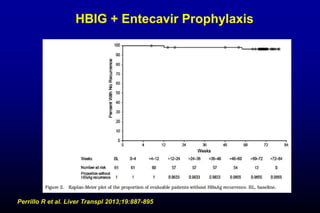
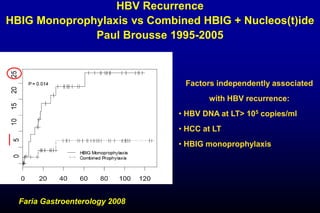
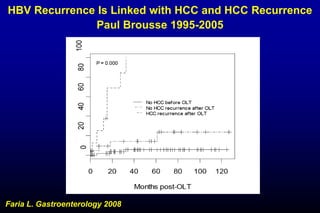
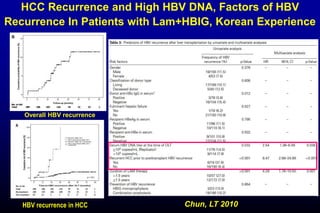
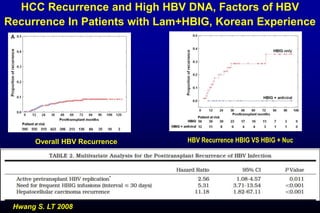
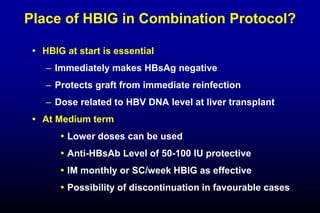
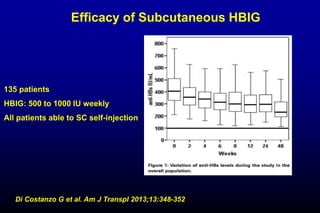
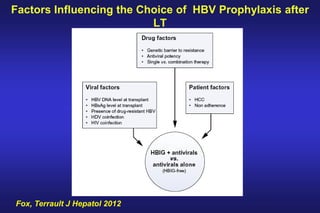
This document discusses optimal strategies for preventing hepatitis B virus (HBV) recurrence after liver transplantation. It reviews evidence that combination prophylaxis with hepatitis B immunoglobulin (HBIG) and nucleoside/nucleotide analogues (NUCs) is most effective at preventing early HBV reinfection. For long-term prophylaxis, low-dose HBIG or HBIG discontinuation combined with lifelong NUC therapy may be sufficient for patients at low risk of recurrence. Factors such as HBV DNA level pre-transplant, hepatocellular carcinoma, and HBV/HIV coinfection increase risk of recurrence and require continued HBIG plus NUC prophylaxis.
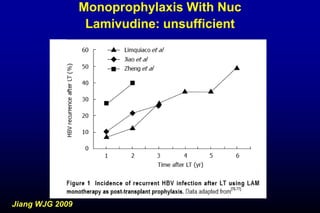
![Monoprophylaxis With Nuc
Lamivudine
Some patients remained HBsAg positive after liver transplant
Progressive decline of HBsAg1
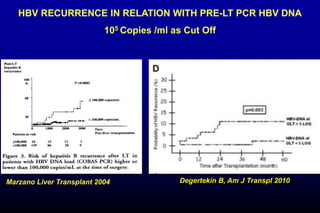
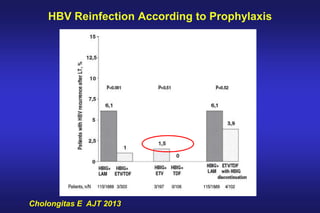
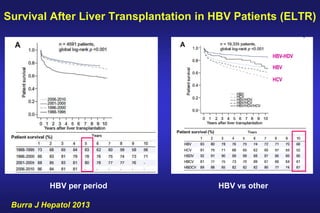
Rate of HBV reinfection
– Related to HBV DNA level before liver transplant
– Related to treatment duration
– Increase with time post-transplant
HBV reinfection due to YMDD HBV mutant
Question of long-term compliance and risk of reinfection
1. Grellier L et al. Lancet. 1996;348:1212 [published correction in Lancet. 1997;349:364]](https://image.slidesharecdn.com/xi71ngxcqv2pr5y9o8ff-signature-6f006525617f2b92773dab668ca306346a0a29494921fcc7056e51c49b86a339-poli-160122161407/85/Samuel1-hbv-lt-du16-13-320.jpg)