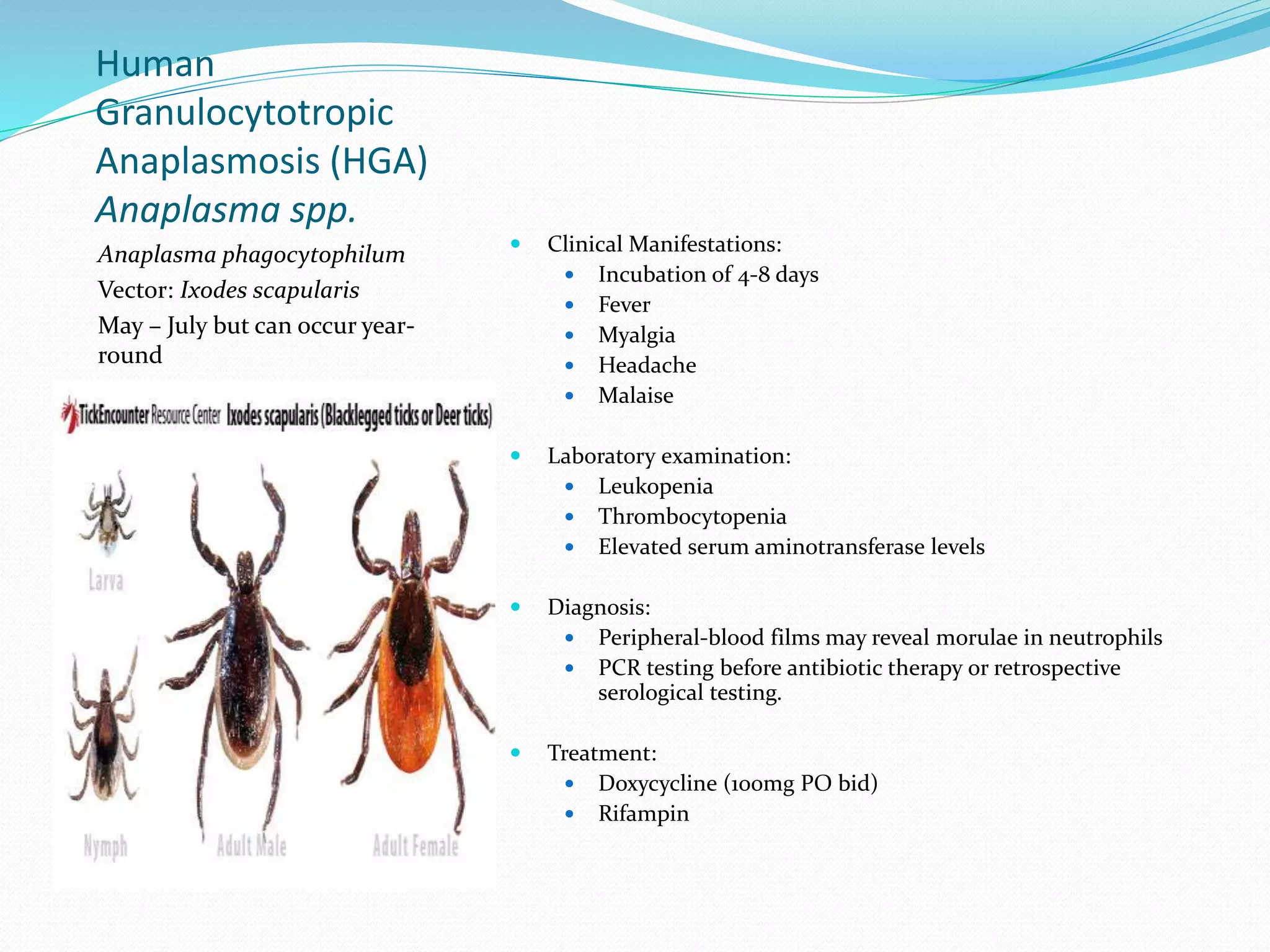
This document summarizes several tick-borne and zoonotic diseases, including their causative agents, vectors, clinical manifestations, diagnosis, and treatment. Granulocytic anaplasmosis is caused by Anaplasma phagocytophilum, transmitted by Ixodes ticks, and presents as fever, myalgia and leukopenia. Ehrlichiosis is caused by Ehrlichia species and presents as nonspecific symptoms like headache and fatigue. Bartonella species cause cat scratch disease from contact with cats, presenting as lymphadenopathy.







































































![Borrelia[231].Presentation MICROBIOLOGY BSMMU](https://cdn.slidesharecdn.com/ss_thumbnails/borrelia231-240320141147-bfe8a2fb-thumbnail.jpg?width=640&height=640&fit=bounds)