Downloaded 53 times














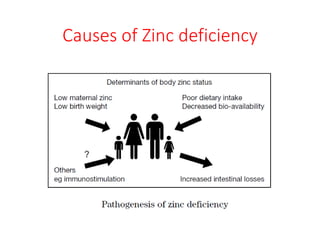





















Zinc deficiency can have serious negative health impacts, especially in children. It is estimated that 25% of the world's population is at risk of zinc deficiency. Zinc plays a critical role in cell metabolism, immunity, growth, and cognitive function. Zinc deficiency increases the risks of prolonged diarrhea, frequent respiratory infections, poor growth and stunting in children under 5 years of age. Treatment of zinc deficiency involves oral zinc supplementation, especially for children with acute diarrhea or those at risk of zinc deficiency due to malnutrition. Preventive measures like zinc supplementation and multiple micronutrient powders can help reduce the risks of zinc deficiency and its associated negative health outcomes in children.























































































