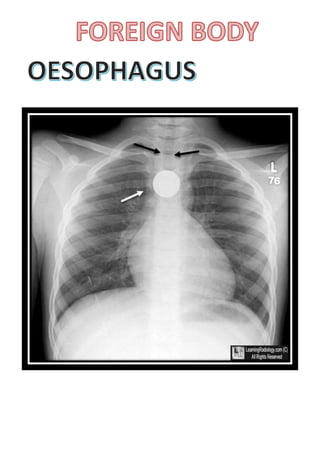
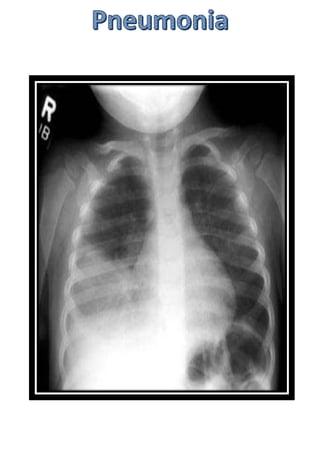
Wilhelm Röntgen discovered X-rays on November 8th, 1895. The first ever X-ray image was of his wife Bertha Röntgen's hand. X-rays provide important diagnostic information for evaluating conditions like pneumonia, fractures, and foreign bodies. Special considerations are needed when performing X-rays on pediatric patients due to their increased radiosensitivity.













































































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











