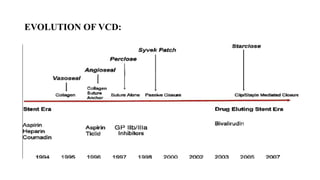
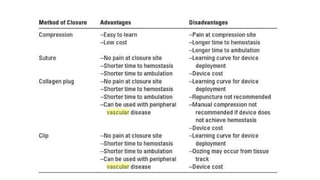
The document discusses the evolution and advantages of vascular closure devices (VCDs) in achieving hemostasis after arterial procedures, emphasizing their utility over traditional manual compression methods. It details various types of VCDs, including active and passive devices, their mechanisms, and comparative outcomes related to complications and recovery times. The document also highlights complications associated with endovascular procedures and patient selection criteria to minimize risks.







































![Invasive_Cardio-Devices_procedures[1].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/invasivecardio-devicesprocedures1-240129085722-eb86cfb0-thumbnail.jpg?width=640&height=640&fit=bounds)



















































