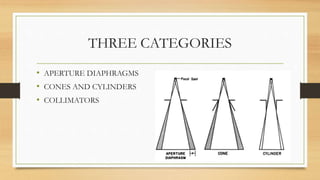
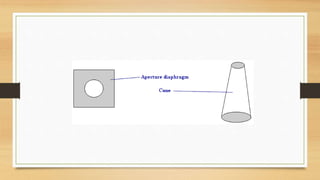
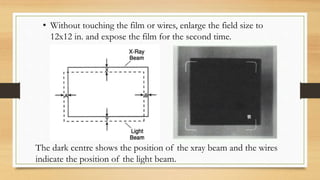
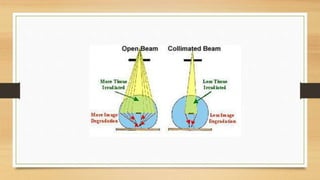
There are three categories of x-ray beam restrictors: aperture diaphragms, cones and cylinders, and collimators. They all function to regulate the size and shape of the x-ray beam. Closely collimating the beam provides two main advantages: it exposes a smaller area of the patient, and it reduces scatter radiation. Properly aligning the light and x-ray beams is important for patient safety and image quality.


















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


















