1. Wound healing is the body's complex biological response to tissue injury. It involves regeneration and repair processes to restore tissue integrity and function.
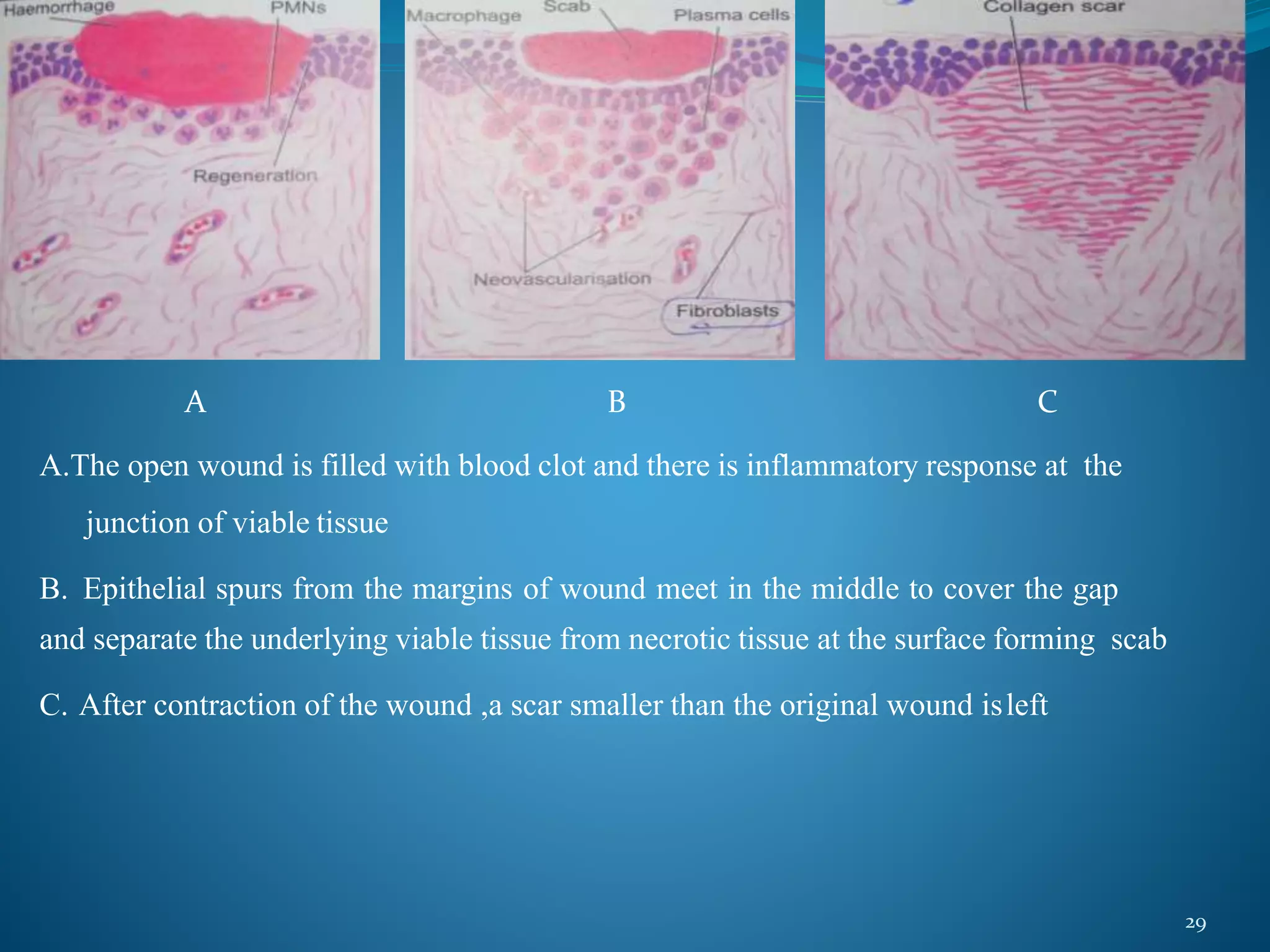
2. There are four main phases of wound healing: hemostasis, inflammation, proliferation, and remodeling. Various cell types and mediators are involved in each phase to clean the wound and promote new tissue growth.
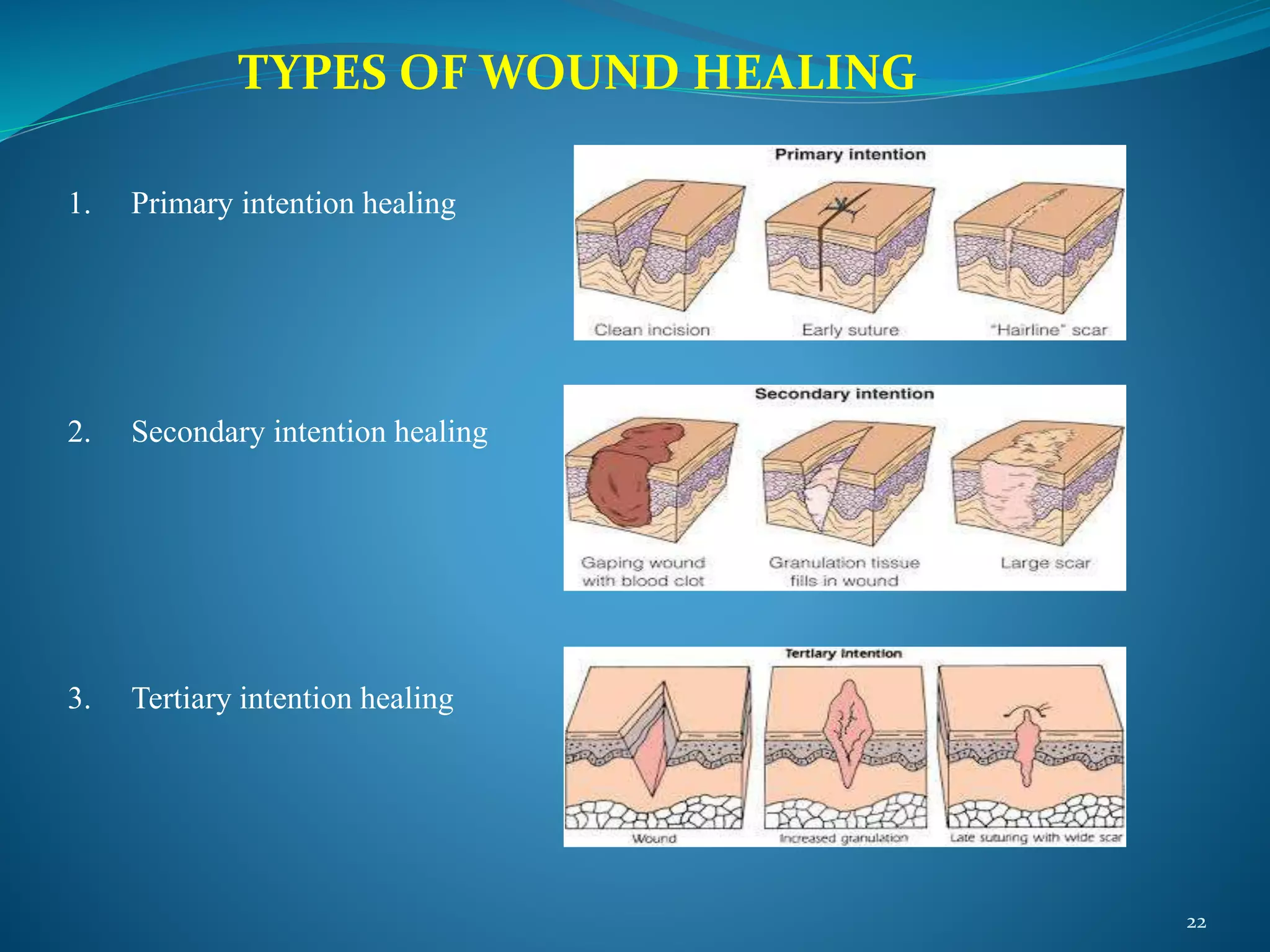
3. Wounds can heal through primary intention, secondary intention, or tertiary intention depending on factors like cleanliness and tissue loss. Primary intention involves direct wound edge approximation while secondary intention involves healing from the base up without suturing.