Download to read offline



![PRACTICE
STANDARDS INCLUDE:
• Nursing Practice according to stat’s Act
• Joint Commission on Accreditation of Healthcare
Organizations (JCAHO)
[if apply]
• Confidentiality
• Informed consent
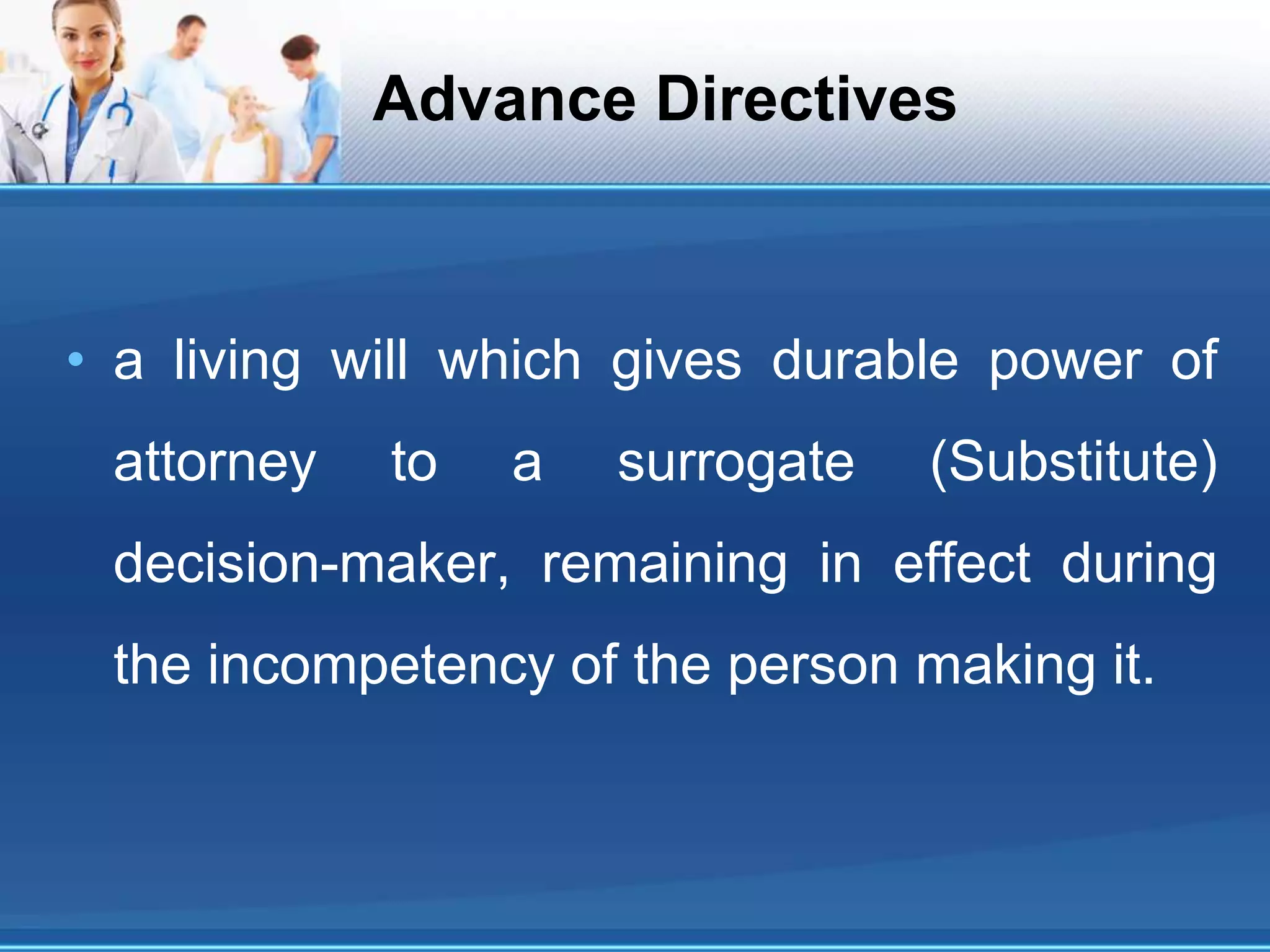
• Advance Directives](https://image.slidesharecdn.com/workshoponncpanddocumentationpimsjehanzebkhan-200625192518/75/WORKSHOP-ON-NCP-AND-DOCUMENTATION-PIMS-JEHANZEB-KHAN-YOUSAFZAI-10-2048.jpg)
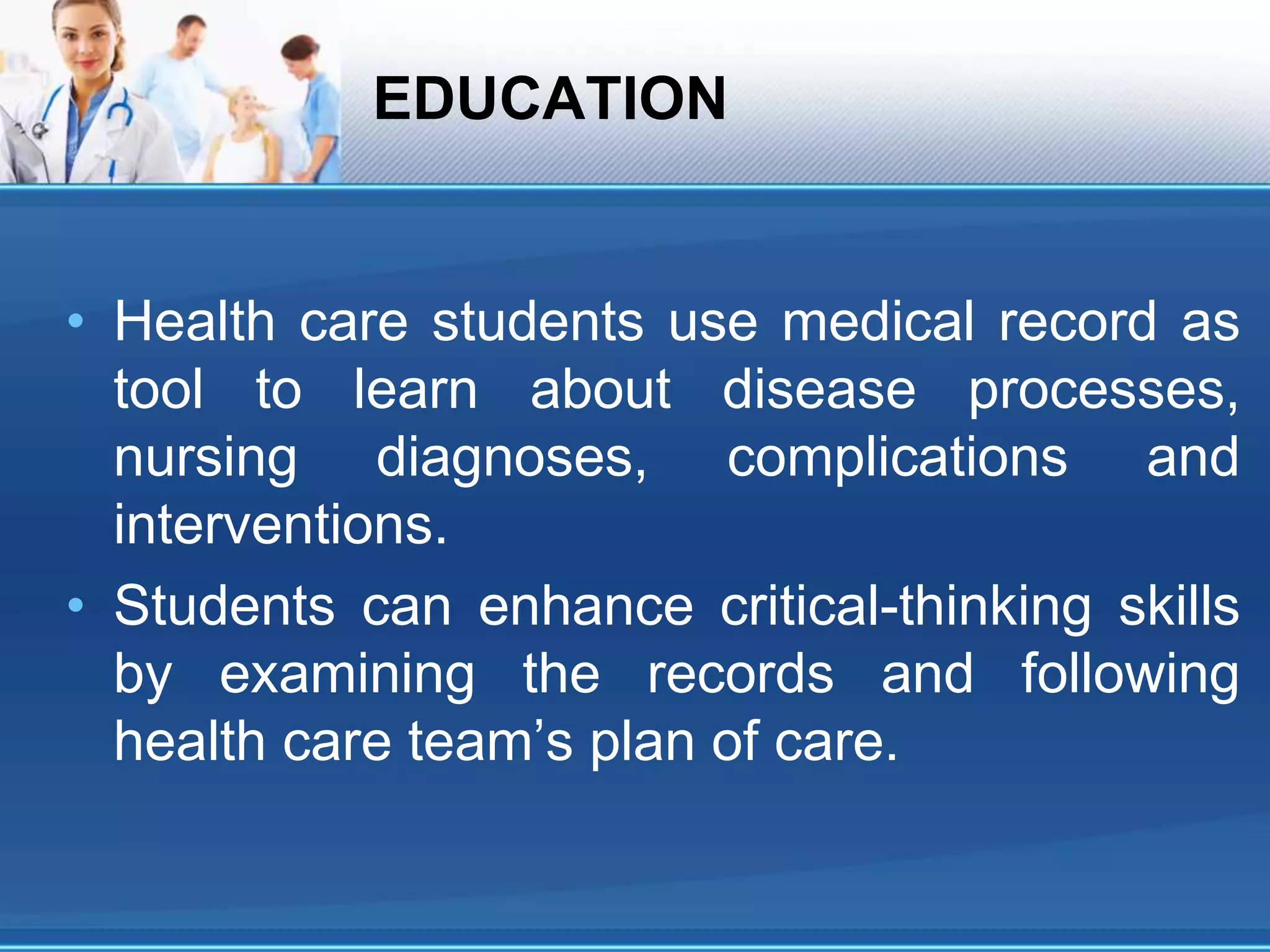



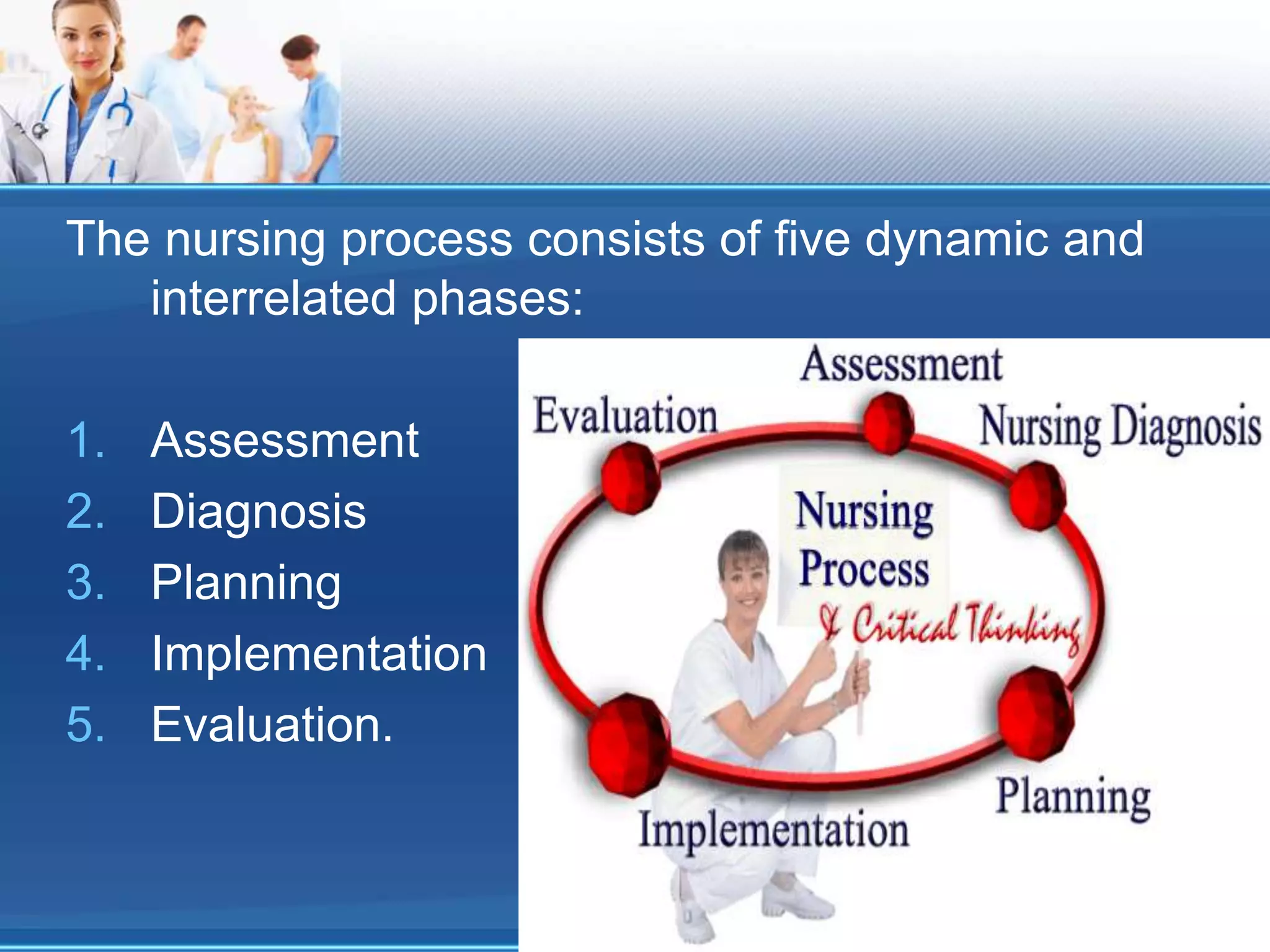
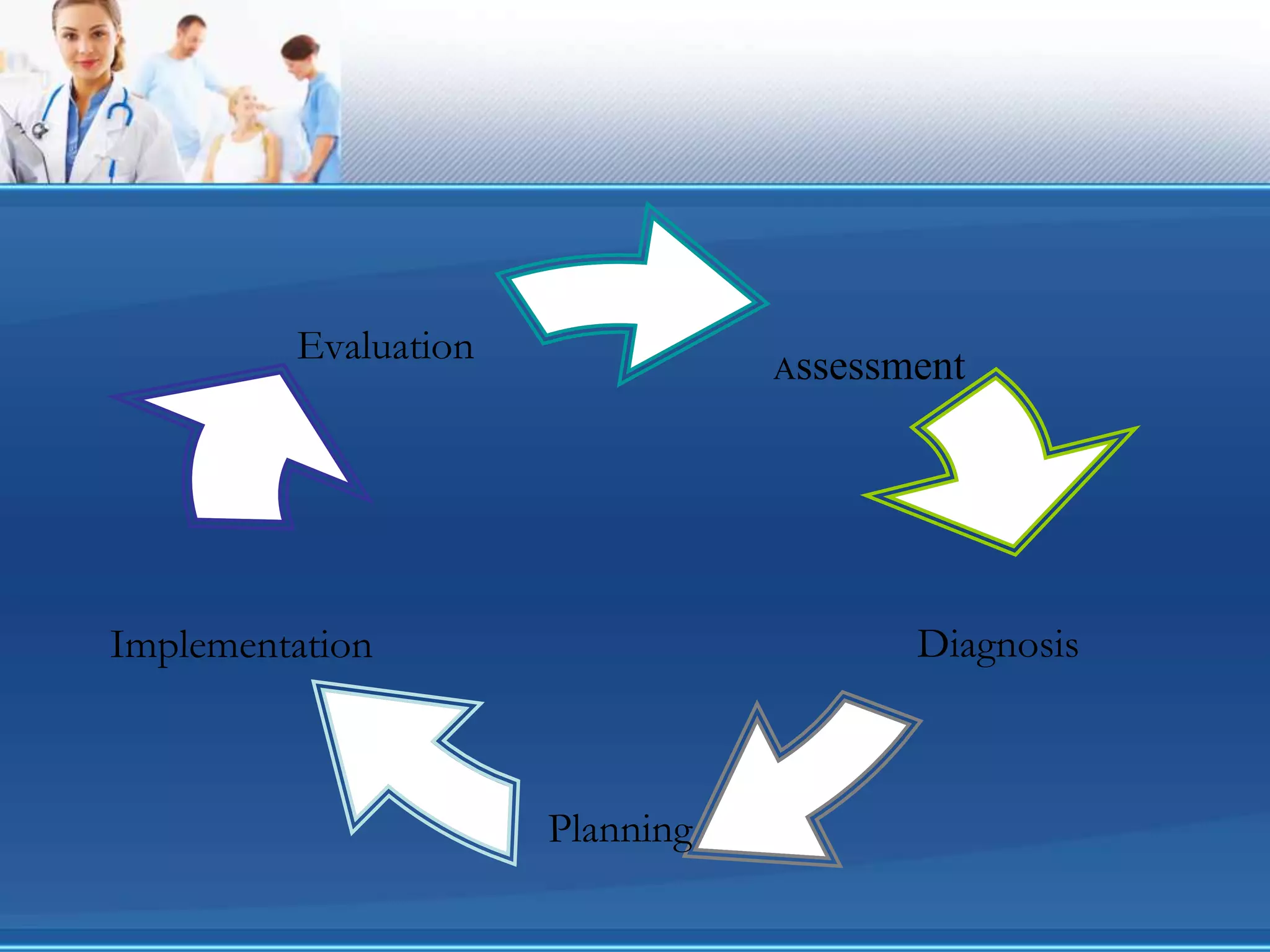
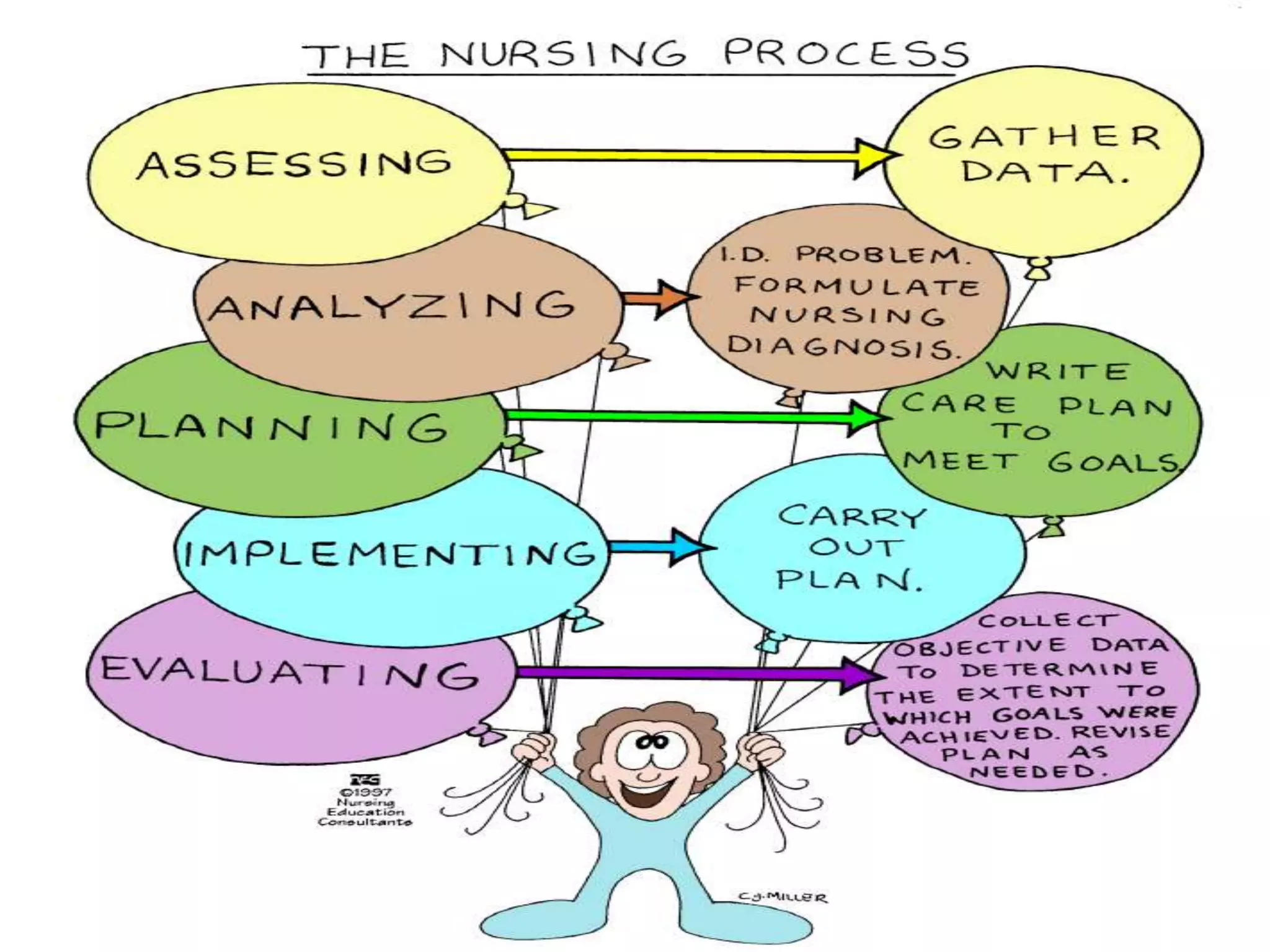



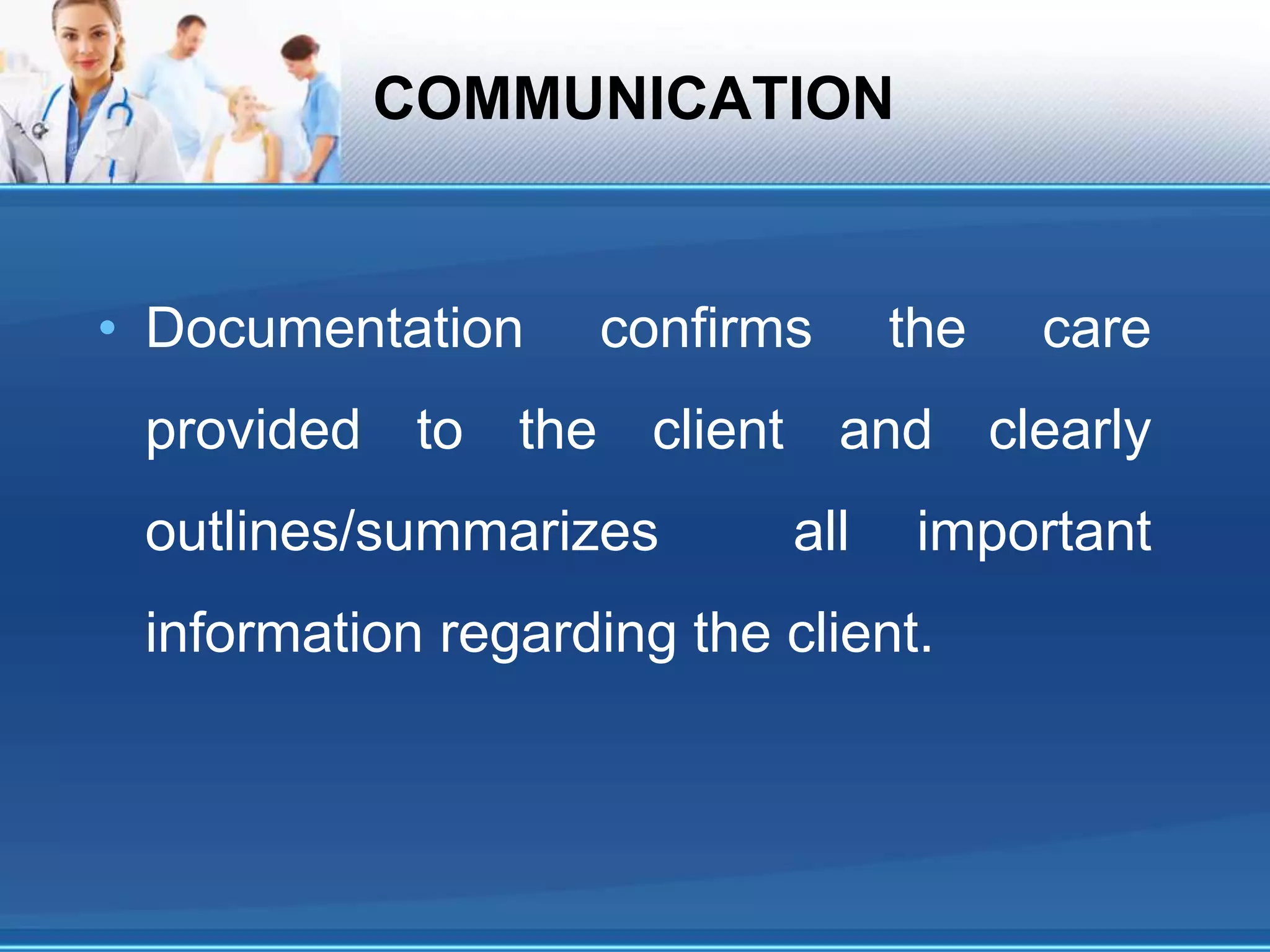
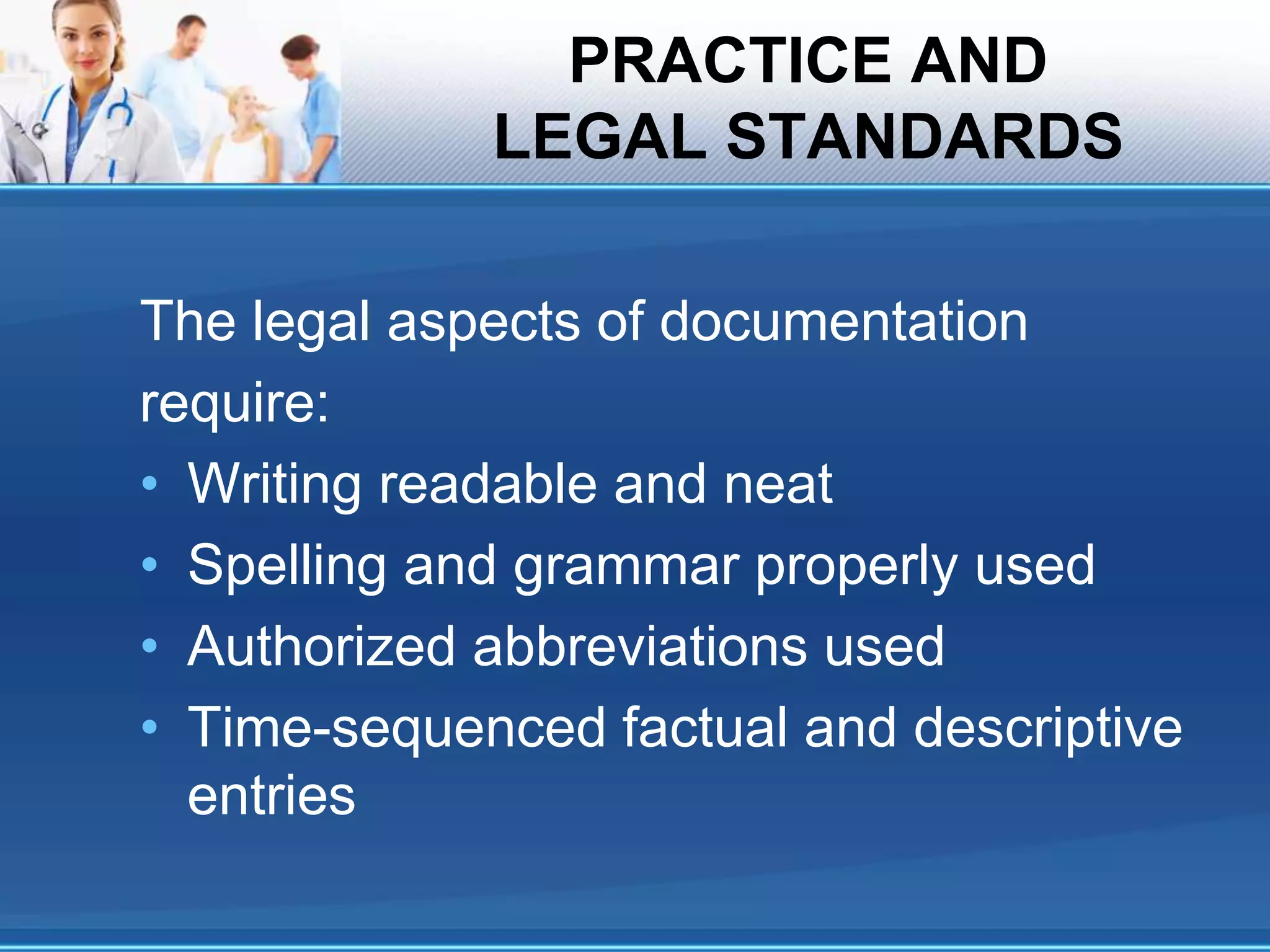
The document outlines the ground rules and objectives for a nursing documentation workshop, detailing the importance of effective documentation in nursing practice. It covers the nursing process, the types of documentation methods, and the principles guiding documentation practices, aiming to enhance communication, legal standards, and education within nursing care. Key focuses include assessment, diagnosis, planning, implementation, and evaluation, emphasizing critical thinking and the legal and ethical responsibilities of nursing professionals.





















































![Understanding Parkinson’s Disease: Causes, Symptoms, and Treatment [2025]](https://cdn.slidesharecdn.com/ss_thumbnails/understandingparkinson-251208102525-80ba3223-thumbnail.jpg?width=640&height=640&fit=bounds)













