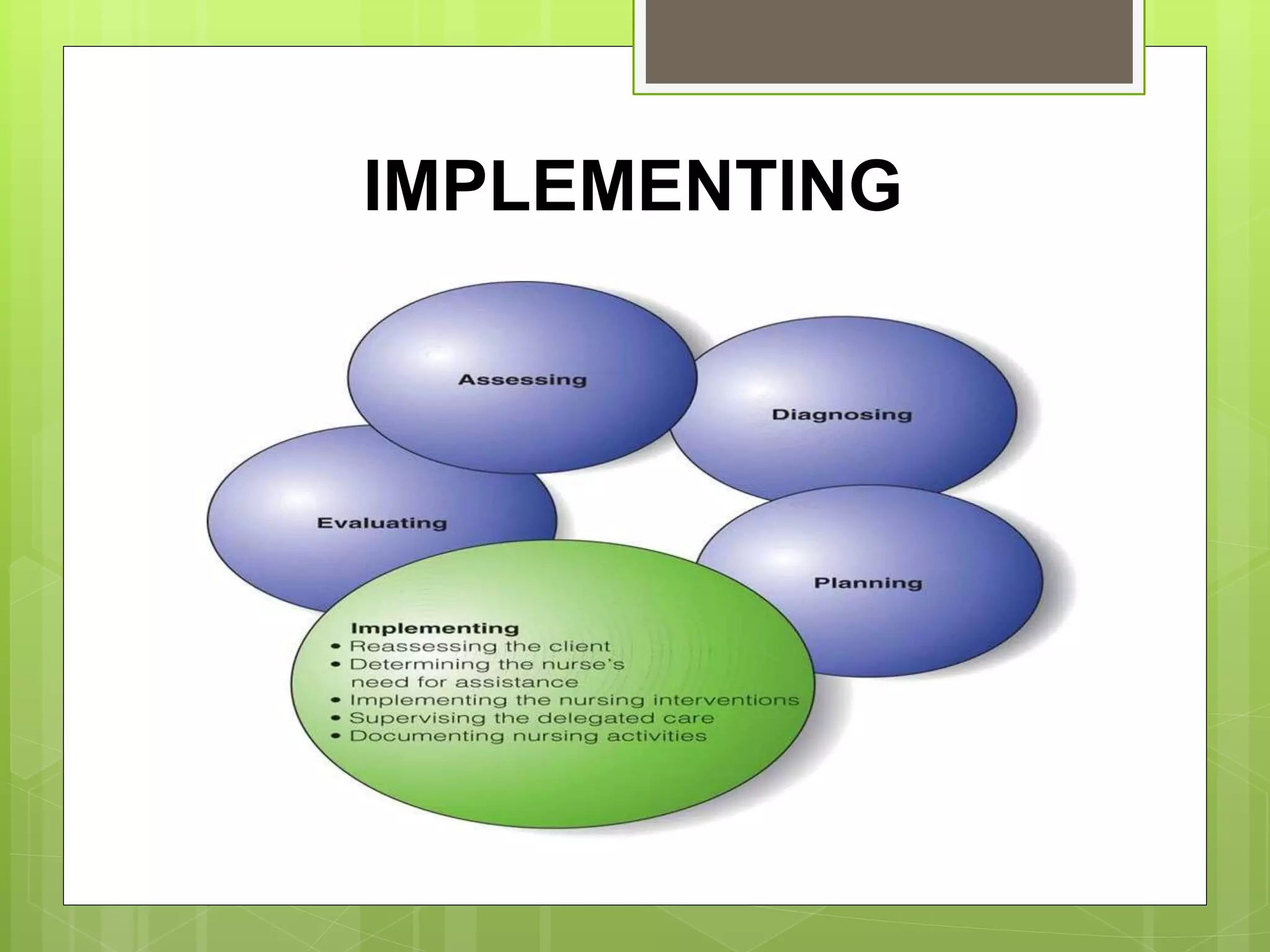
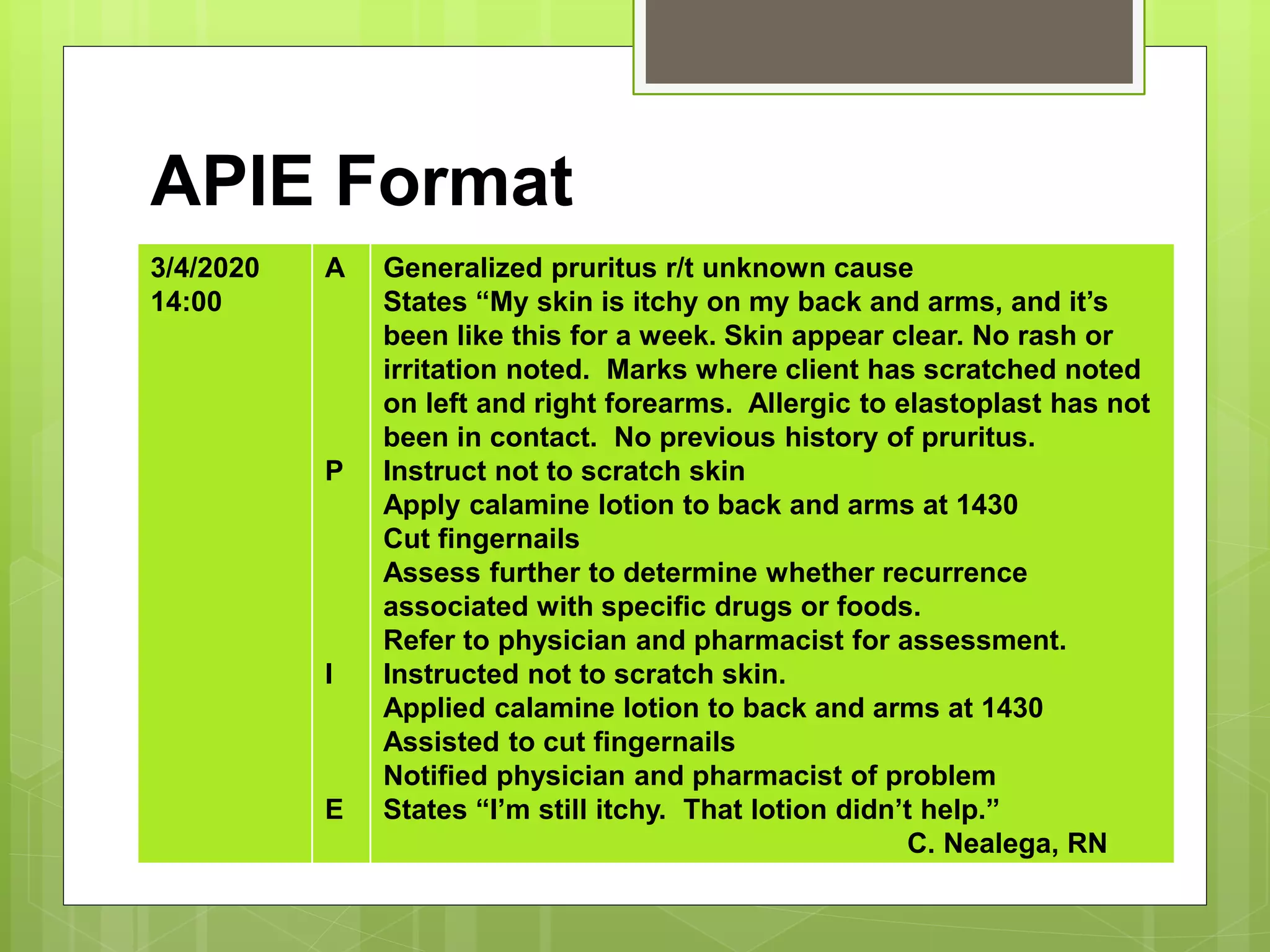
This document discusses the implementation phase of the nursing process. It describes implementing skills like cognitive, interpersonal, and technical skills. The process of implementing includes reassessing the client, determining if assistance is needed, implementing interventions, supervising delegated care, and documenting activities. Guidelines for implementing interventions include basing care on evidence, adapting to individual clients, ensuring safety, and encouraging client participation. The document also discusses different documentation systems like source-oriented records, problem-oriented records, and SOAP/APIE notes.