Downloaded 10 times





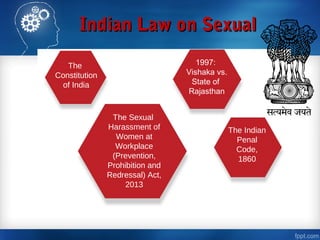



The document discusses various challenges faced by nurses in the workplace including workplace violence, staffing shortages, long working hours, and a lack of recognition. It also provides solutions to address these issues such as implementing positive work environments, improving teamwork, balancing workloads, and recruiting and retaining more staff. The document also outlines Indian laws related to occupational health and safety for nurses, including the National Policy on Safety, Health and Environment at Workplace from 2009 and various labor acts.

























































