Download as PDF, PPTX
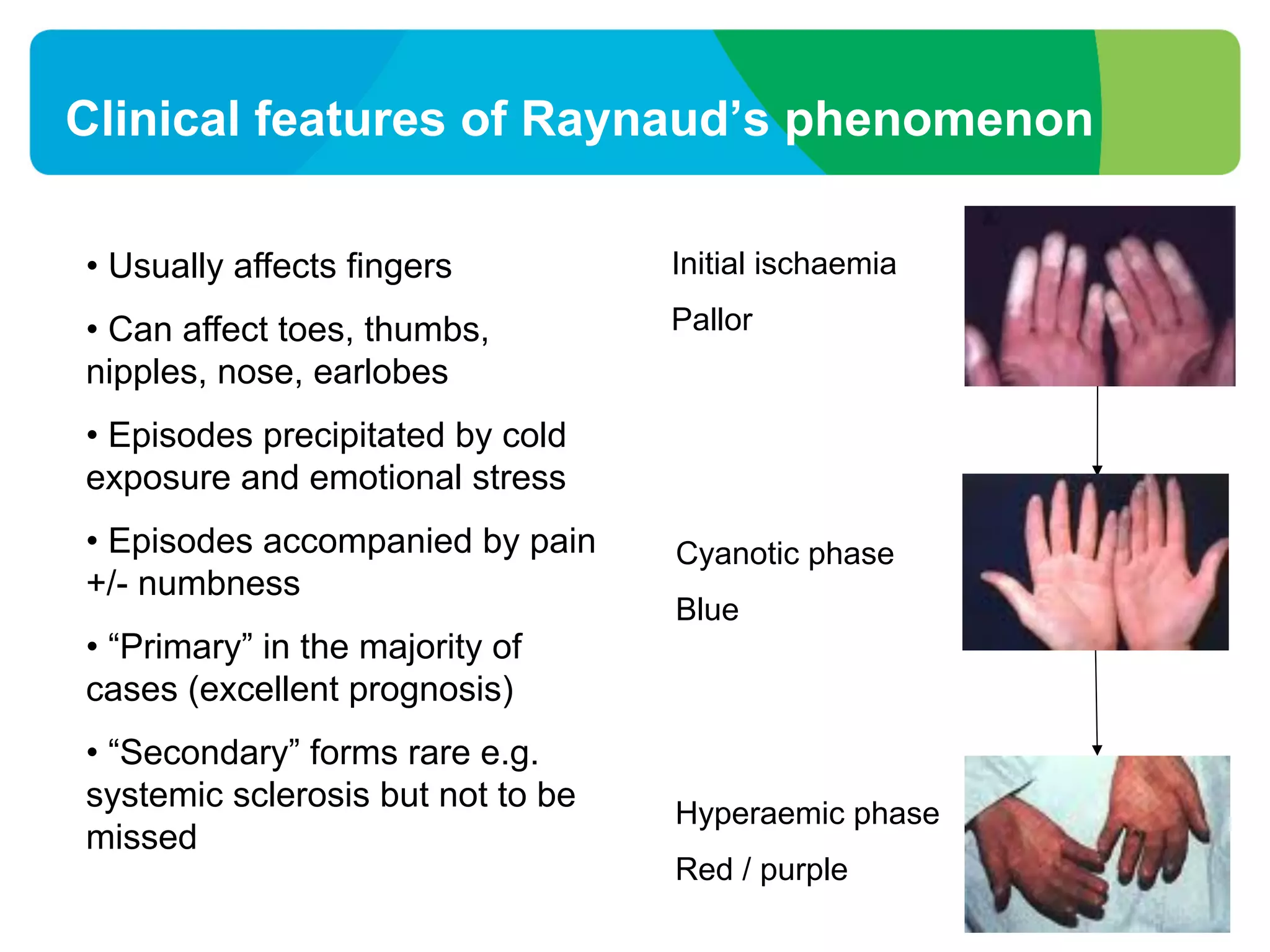

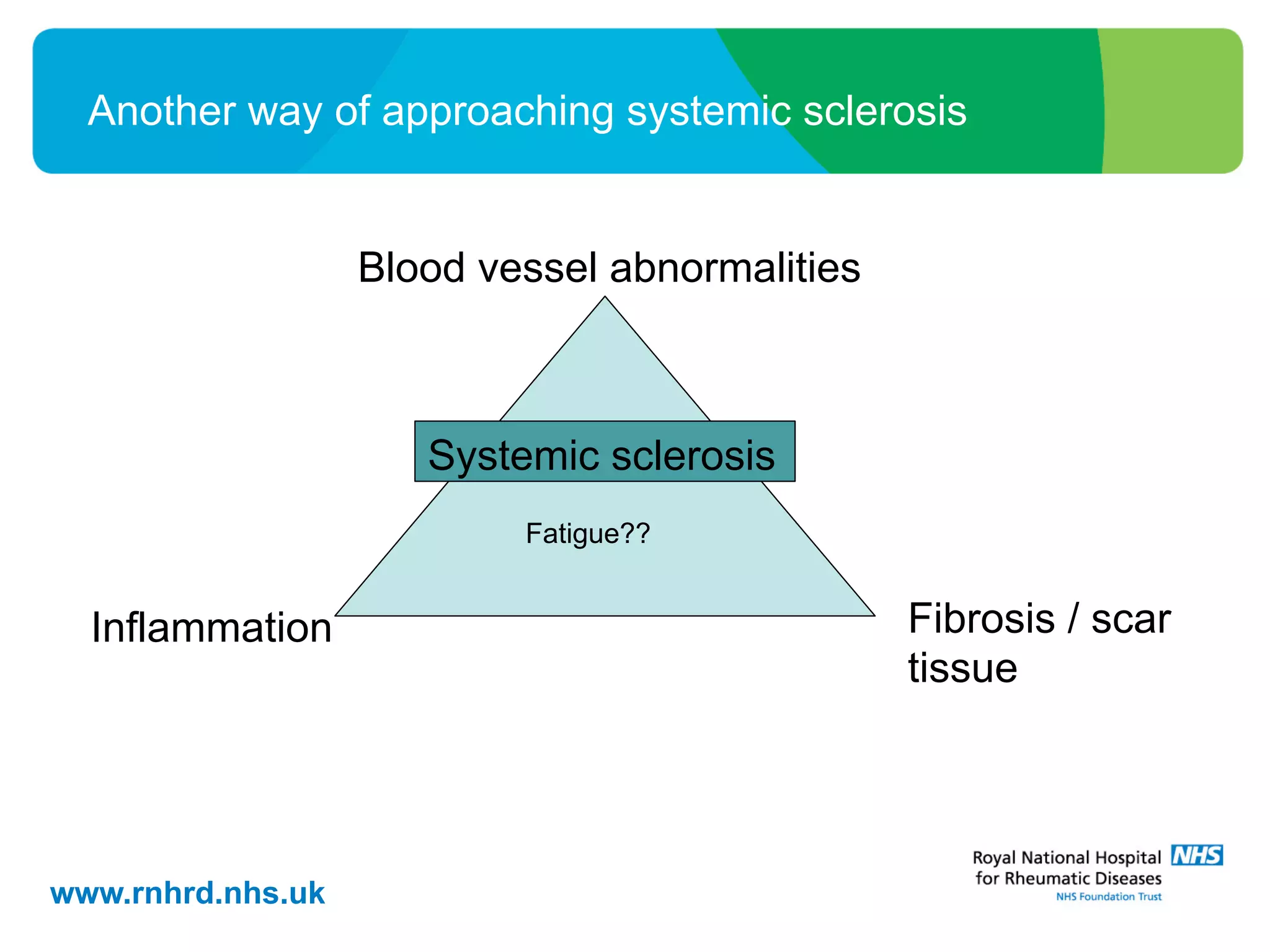
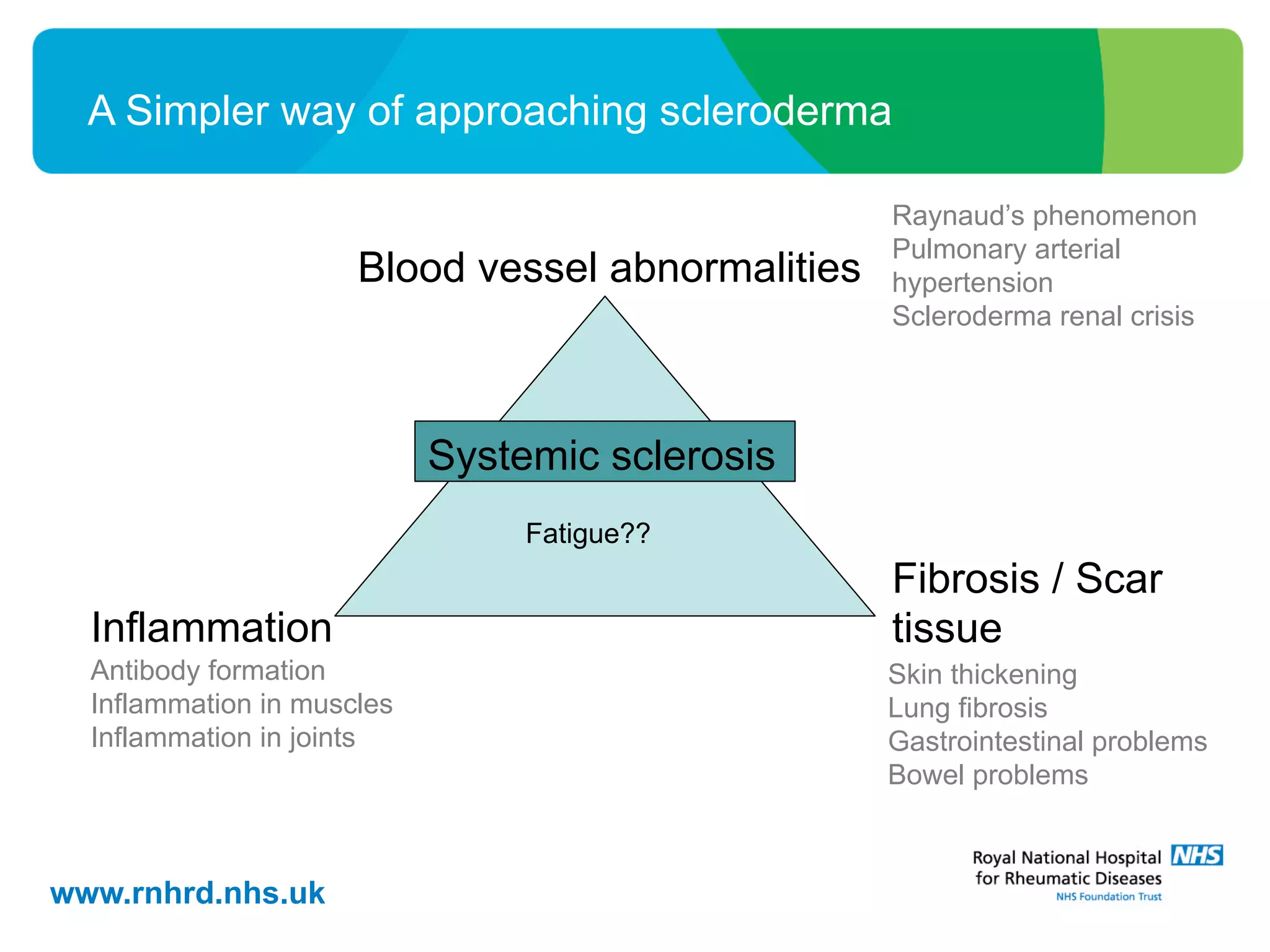
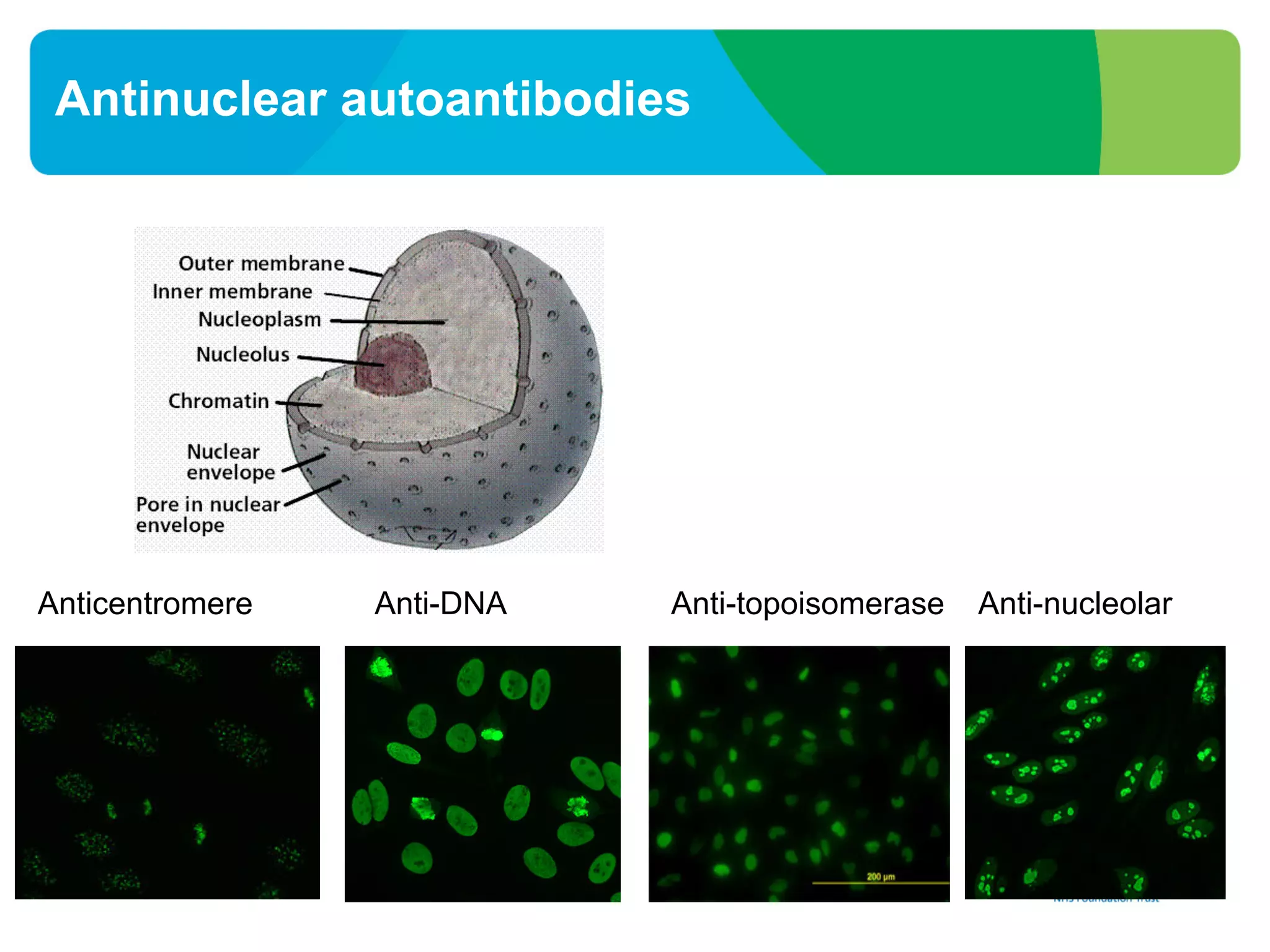
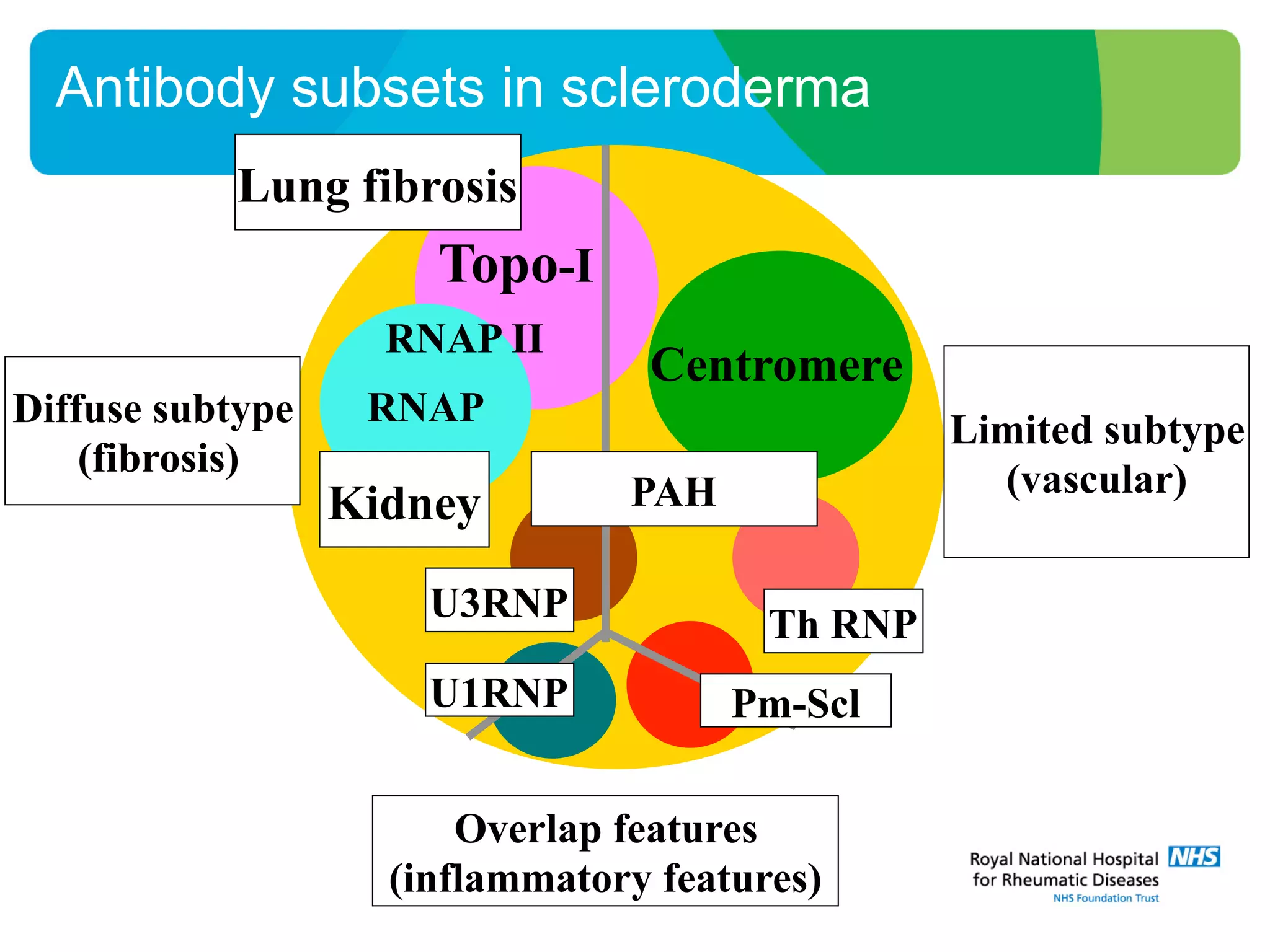
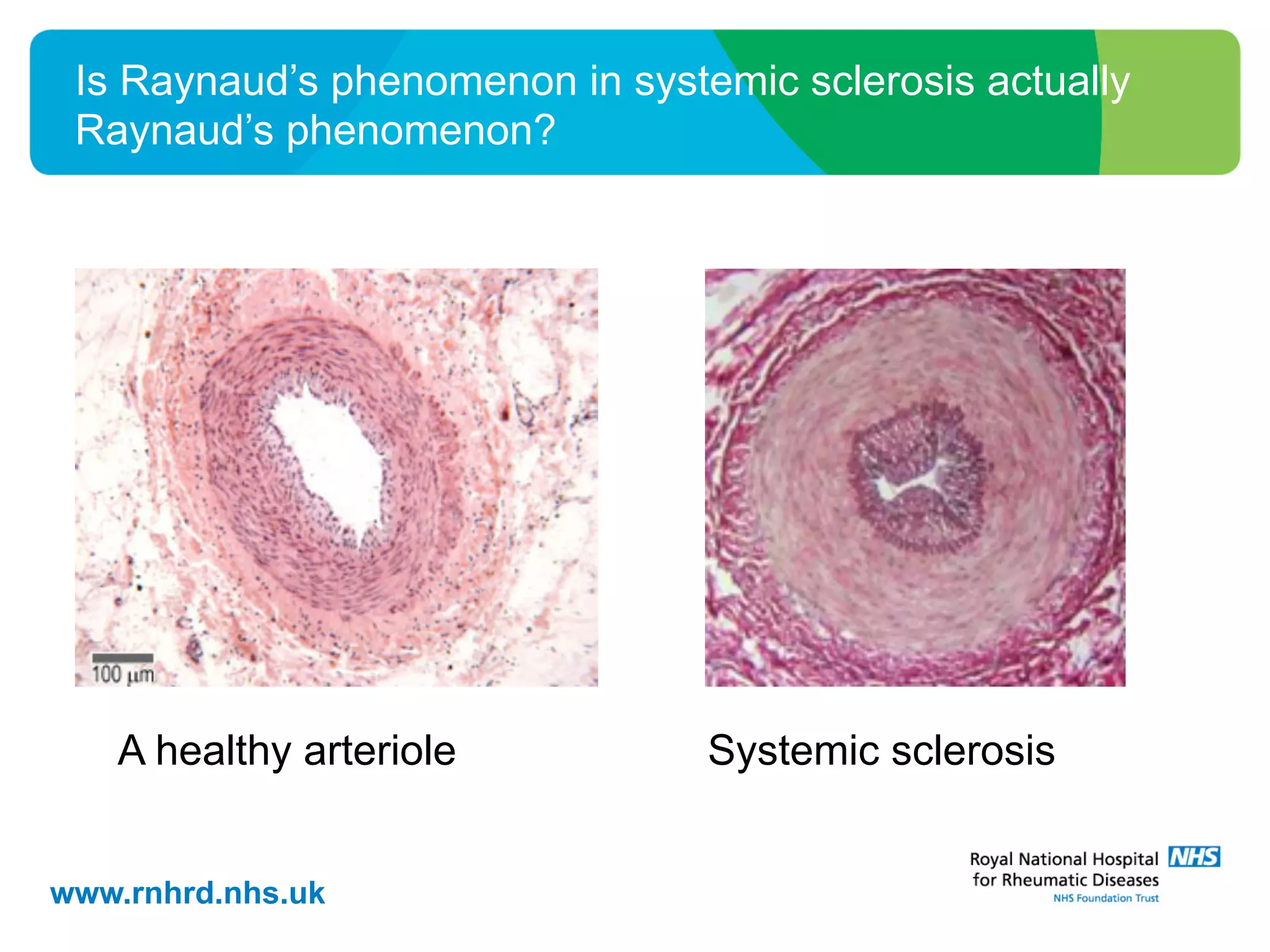
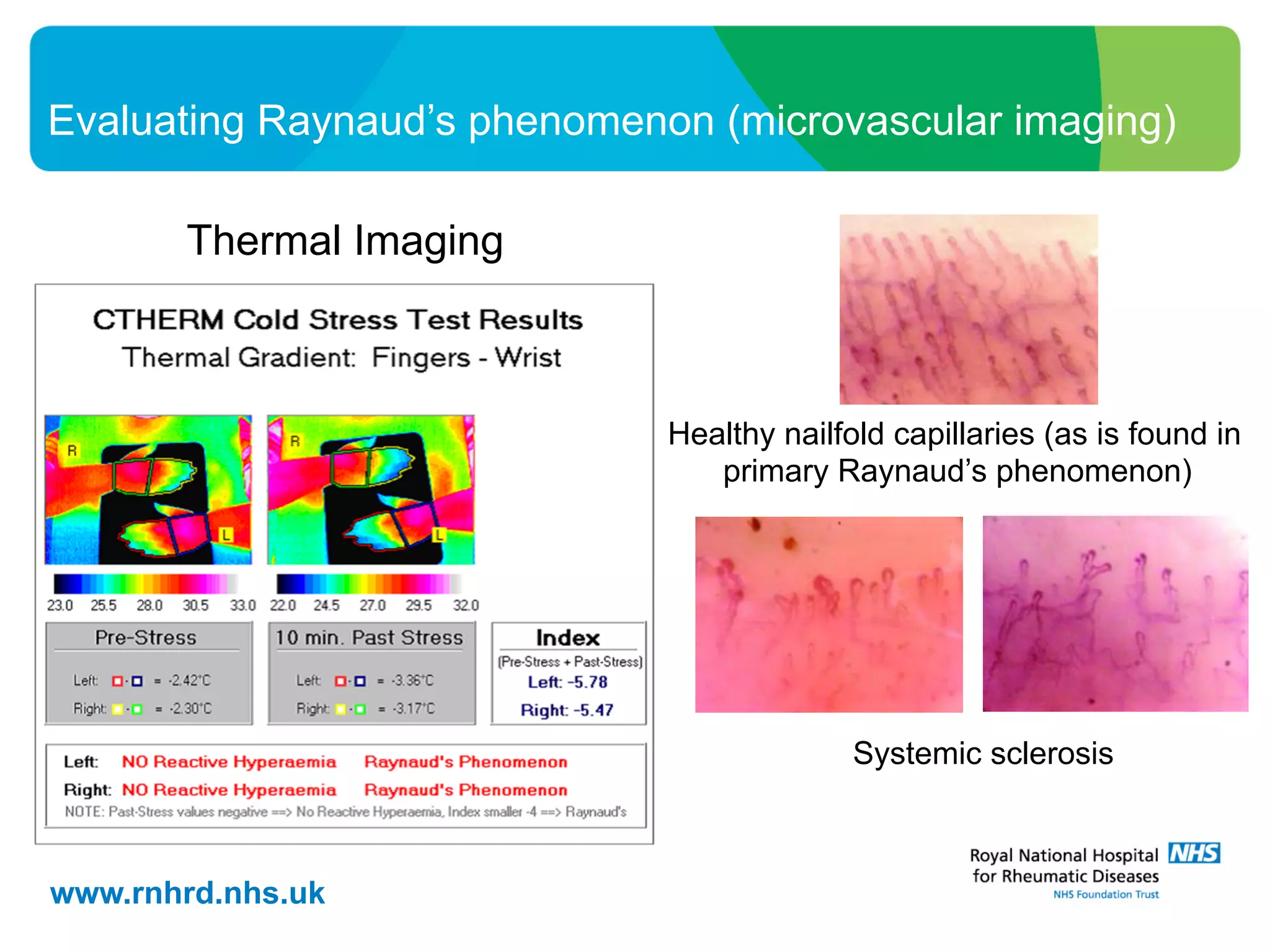
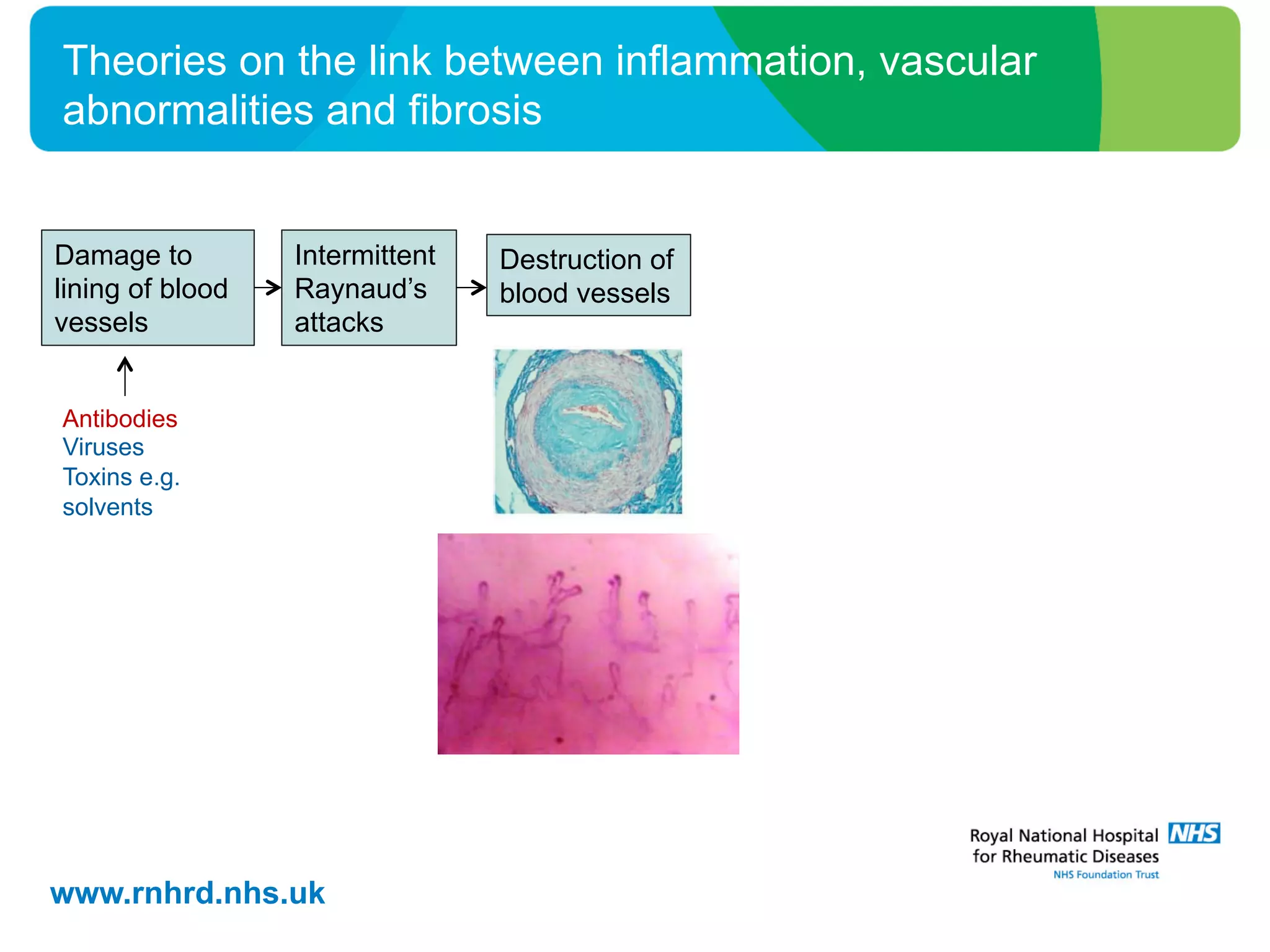
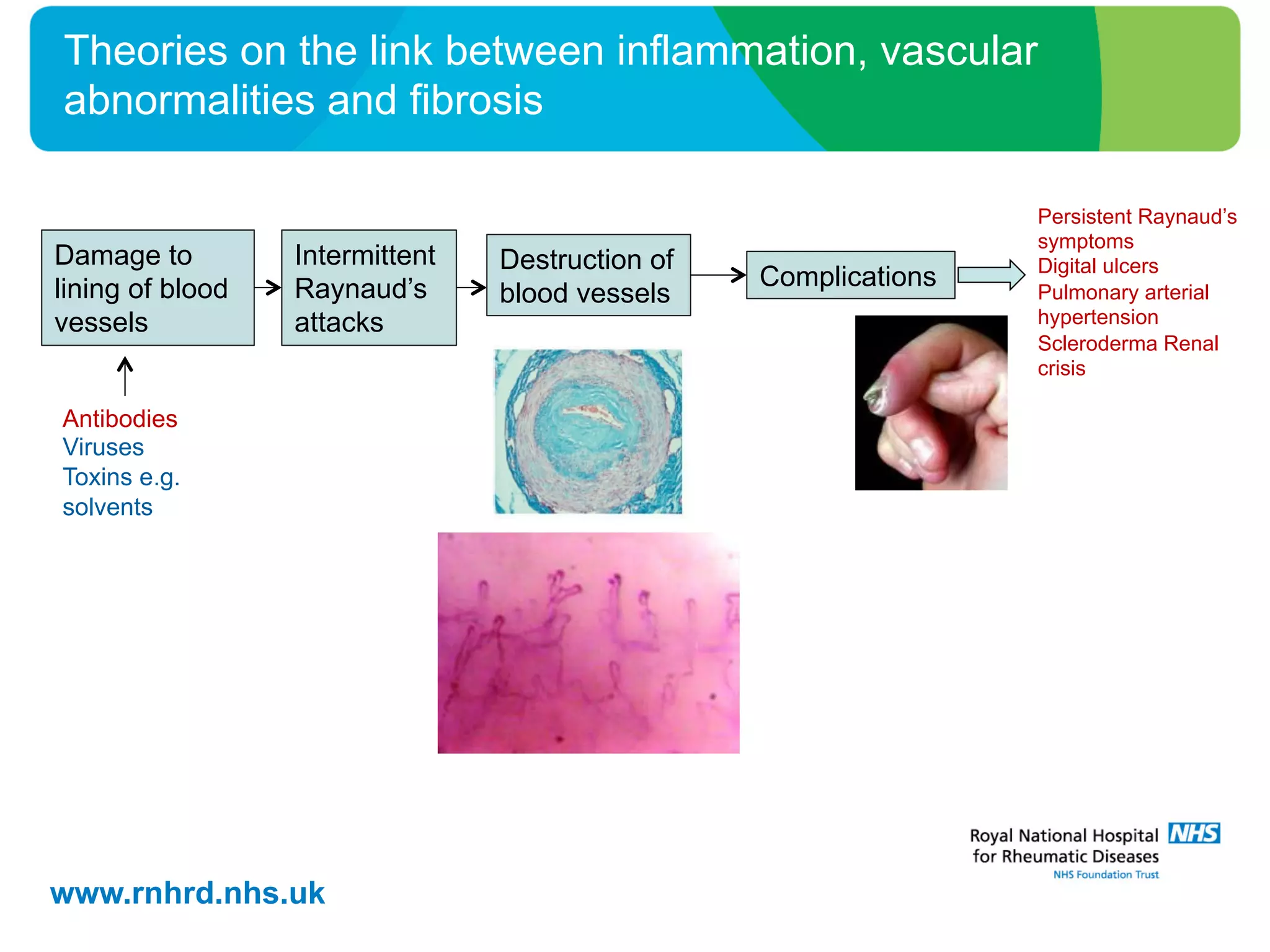
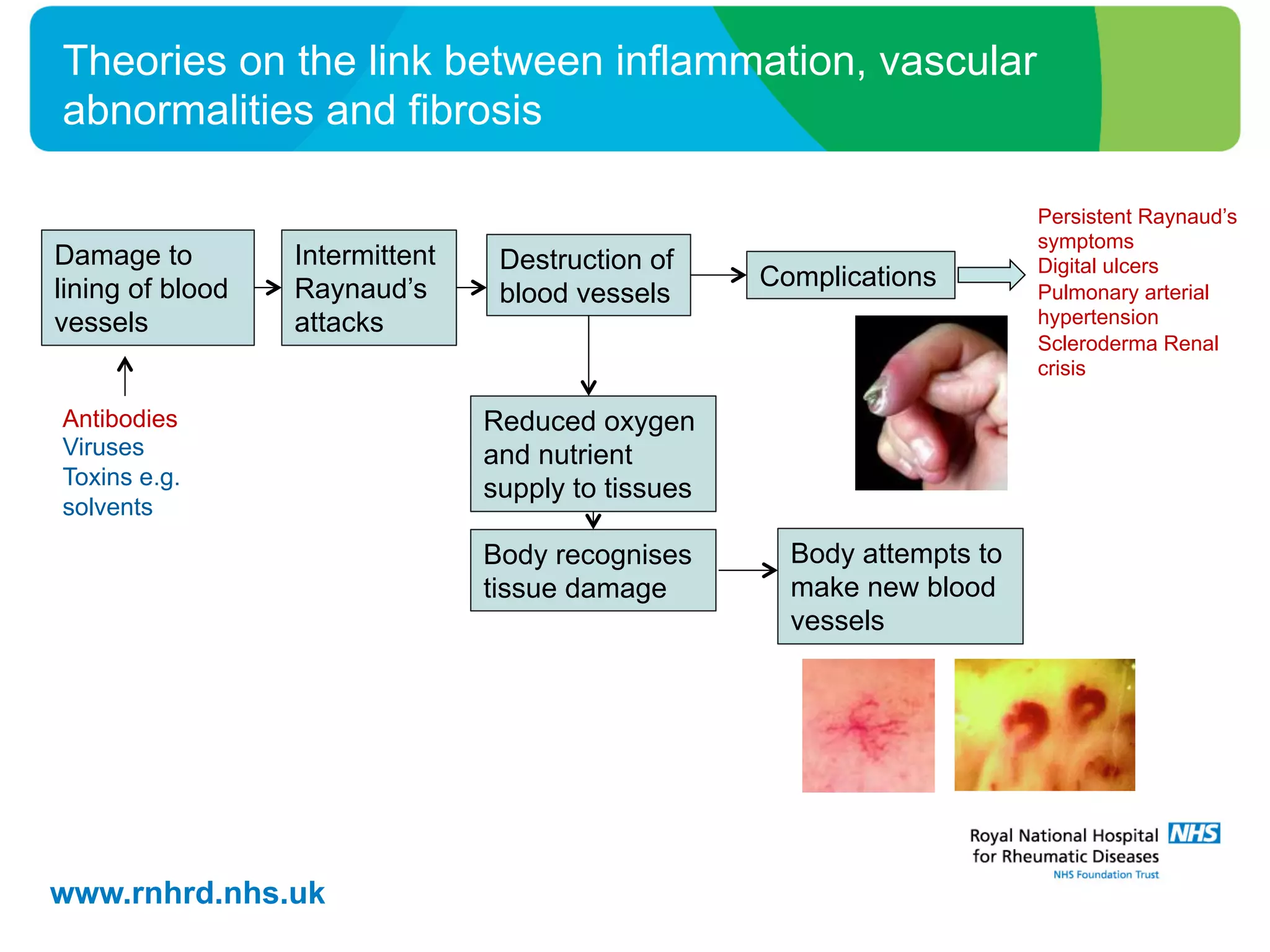
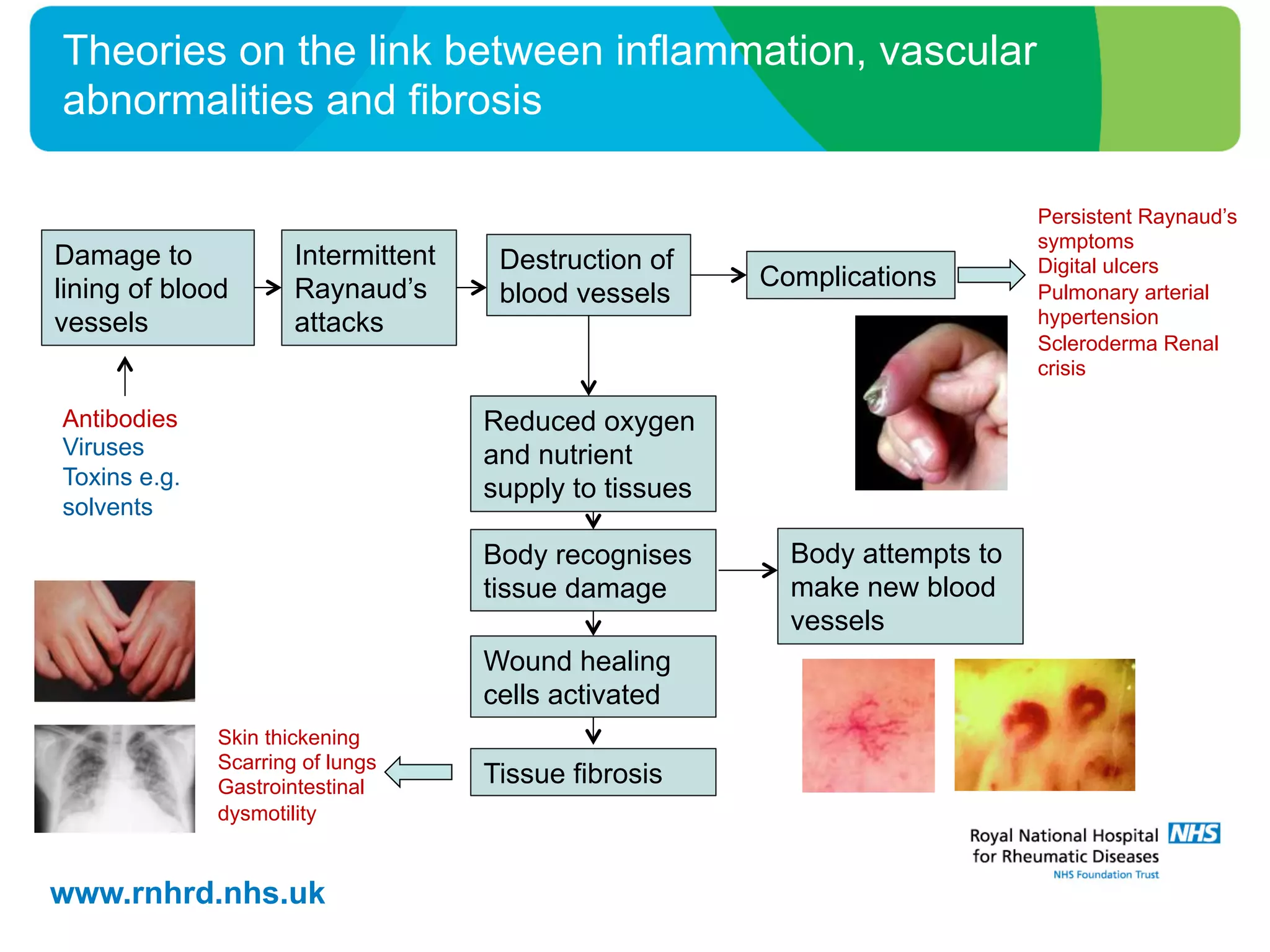

Raynaud's phenomenon and scleroderma are linked vascular conditions. Raynaud's involves reduced blood flow to the extremities while scleroderma causes fibrosis of skin and organs. Damage to blood vessels from Raynaud's attacks may trigger antibodies, inflammation, and attempts to repair tissue through fibrosis. Understanding these pathways could help guide new treatments to prevent complications like lung scarring and kidney or lung failure.









































































