Download to read offline
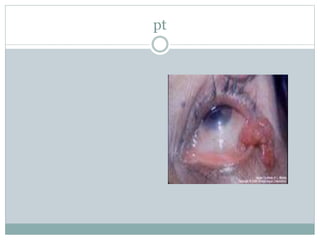
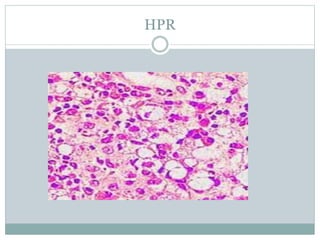

This document discusses two diseases - rhinosporidiosis and rhinoscleroma. Rhinosporidiosis is caused by Rhinosporidium seeberi and presents as a fleshy polypoidal nasal mass that can spread to other sites. It has a life cycle involving trophic, sporangial and endospore stages. Rhinoscleroma is caused by Klebsiella rhinoscleromatis and starts in the nose, potentially spreading to other sites. It has four stages from catarrhal rhinitis to stenotic nasal obstruction. Both diseases are diagnosed by biopsy and treated with surgery and antibiotics.












































































