1. This document discusses surgical approaches for treating type A aortic dissection, including a hybrid approach combining surgery and stenting.
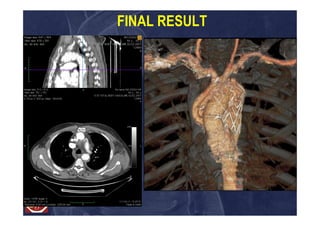
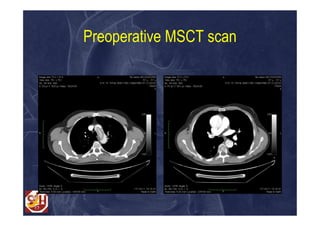
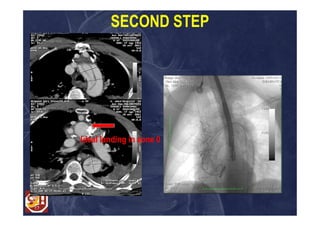
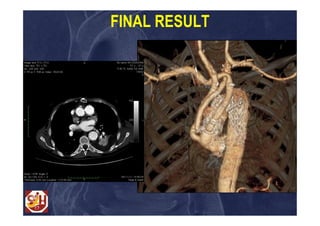
2. It presents two clinical cases where different surgical strategies were used - a multibranched frozen elephant trunk procedure and a two-step approach combining ascending-arch repair with later TEVAR.
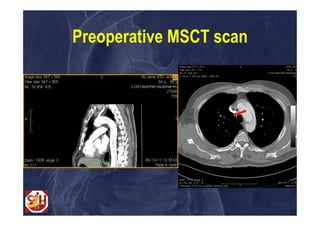
3. The key decision points for surgical treatment are the clinical presentation, site of the intimal tear, and patient age, and the document advocates for extensive aortic repair to prevent chronic enlargement of the false lumen and further complications.