Download as PDF, PPTX
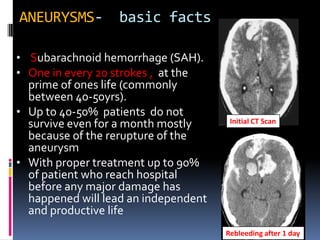
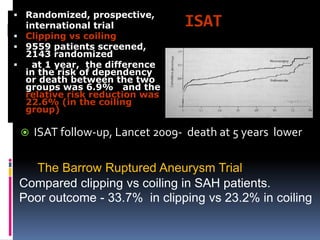
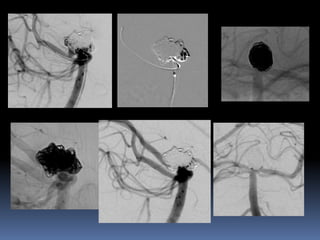
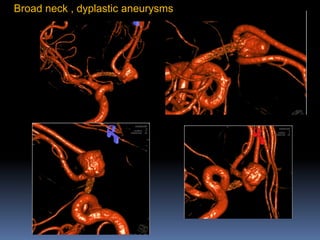
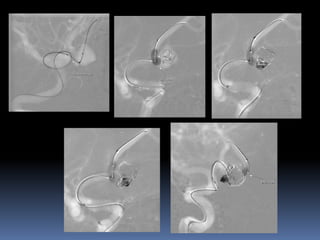
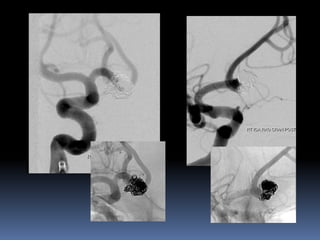
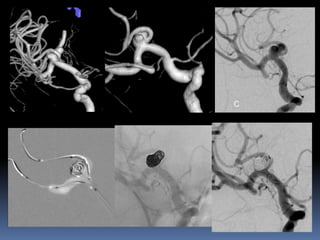
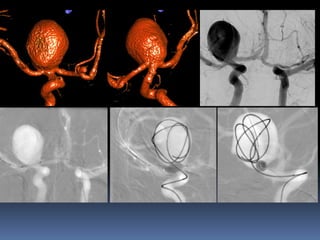
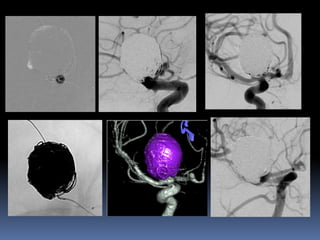

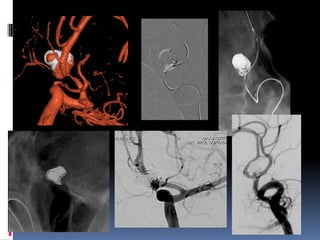
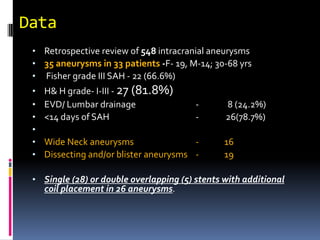




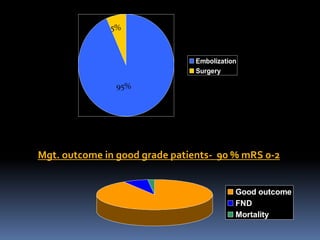
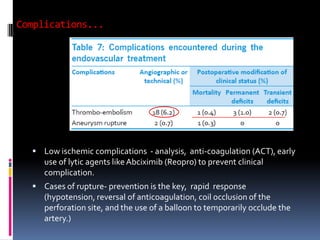
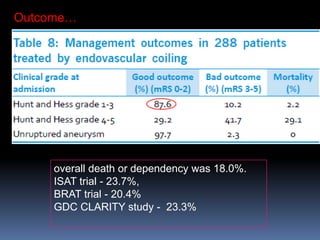
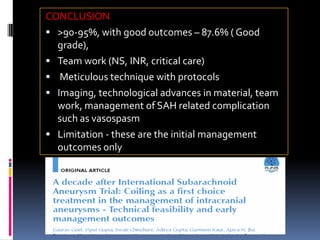


Endovascular coiling is now the primary treatment approach for ruptured intracranial aneurysms based on evidence from trials like ISAT showing improved outcomes compared to clipping. The presenter's experience with 33 patients with 35 consecutive aneurysms showed high rates of aneurysm occlusion (95%) and good clinical outcomes (87.6% had mRS 0-2) when treated using a protocol-based endovascular approach with neurosurgical and critical care support. Complications were low when meticulous techniques were used along with protocols for management of issues like vasospasm.