




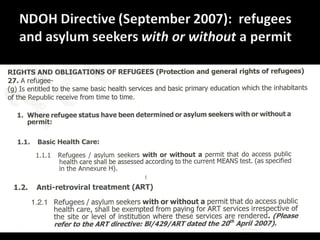
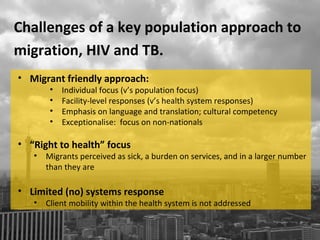


This document discusses migration and health in South Africa. It argues that a "key populations" approach, which views migrants as a homogenous group and exceptionalizes their needs, has unintended negative consequences. Instead, it advocates for a "migration aware" approach that embeds migration as a key social process and considers the heterogeneity of migrant populations. A migration aware approach would support mobility-sensitive health systems, spatially sensitive responses, and continuity of care for both internal and cross-border movement. Properly implementing laws regarding migrants' right to health could improve outcomes for all.


































































