


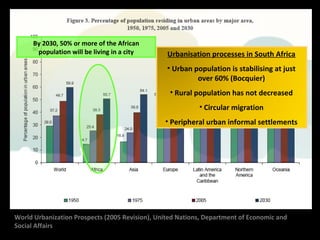

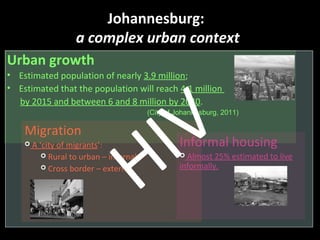
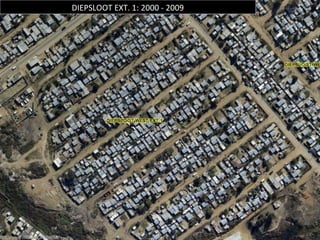
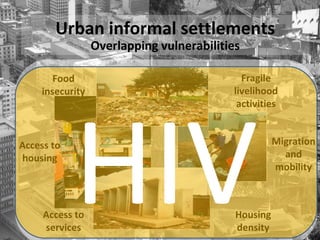
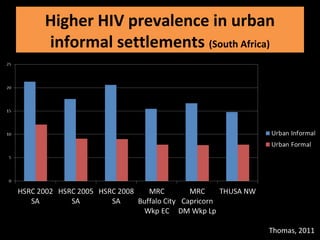
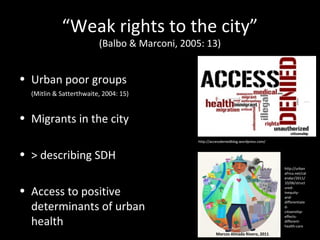
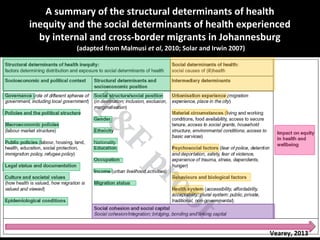
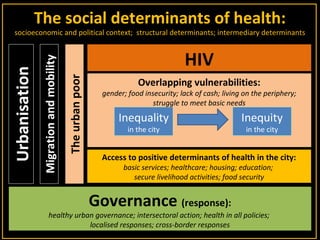

This document discusses migration, inequality, and urban health in Southern African cities. It first provides context on urban growth, migration patterns, and health inequities across diverse Southern African Development Community (SADC) contexts. It then focuses on Johannesburg as a case study, noting its complex urban dynamics including high levels of inequality, migration, and informal settlements which experience overlapping vulnerabilities and higher HIV prevalence. The document calls for actions like healthy urban governance, intersectoral collaboration, localized responses, pro-poor policies, and cross-border cooperation to better address the social determinants of health and reduce inequities experienced by urban poor groups.











![Public health genom[1]](https://cdn.slidesharecdn.com/ss_thumbnails/publichealthgenom1-131004072144-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)














































































