Download to read offline
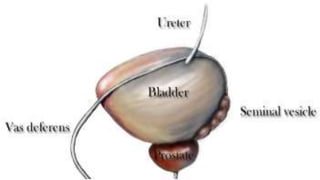
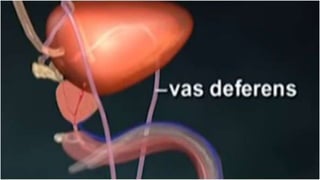
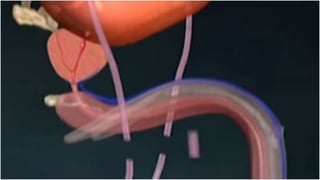








This document provides information about the procedure for a vasectomy. It begins by describing the vas deferens and how interrupting or obstructing this duct inhibits sperm production. It then discusses that a vasectomy is an outpatient surgical procedure where a small segment of the vas deferens is removed and the ends are sealed to prevent sperm from passing through. The preparation of the patient, skin preparation, draping, equipment, instrumentation, supplies and special considerations for the procedure are outlined in detail.























































































