Downloaded 302 times
































![PHACE syndrome
The neurocutaneous
disorder characterized by
posterior fossa
abnormalities [P], large
facial hemangiomas [H],
arterial anomalies [A],
cardiac defects [C], and
eye anomalies [E]
Frieden IJ, Reese V, Cohen D. PHACE syndrome. The association of posterior fossa brain malforma- tions, hemangiomas, arterial
anomalies, coarctation of the aorta and cardiac defects, and eye abnormal- ities. Arch Dermatol 1996;132(3):307–11.](https://image.slidesharecdn.com/vasculartumors-140911182647-phpapp01/75/Vascular-tumors-34-2048.jpg)






















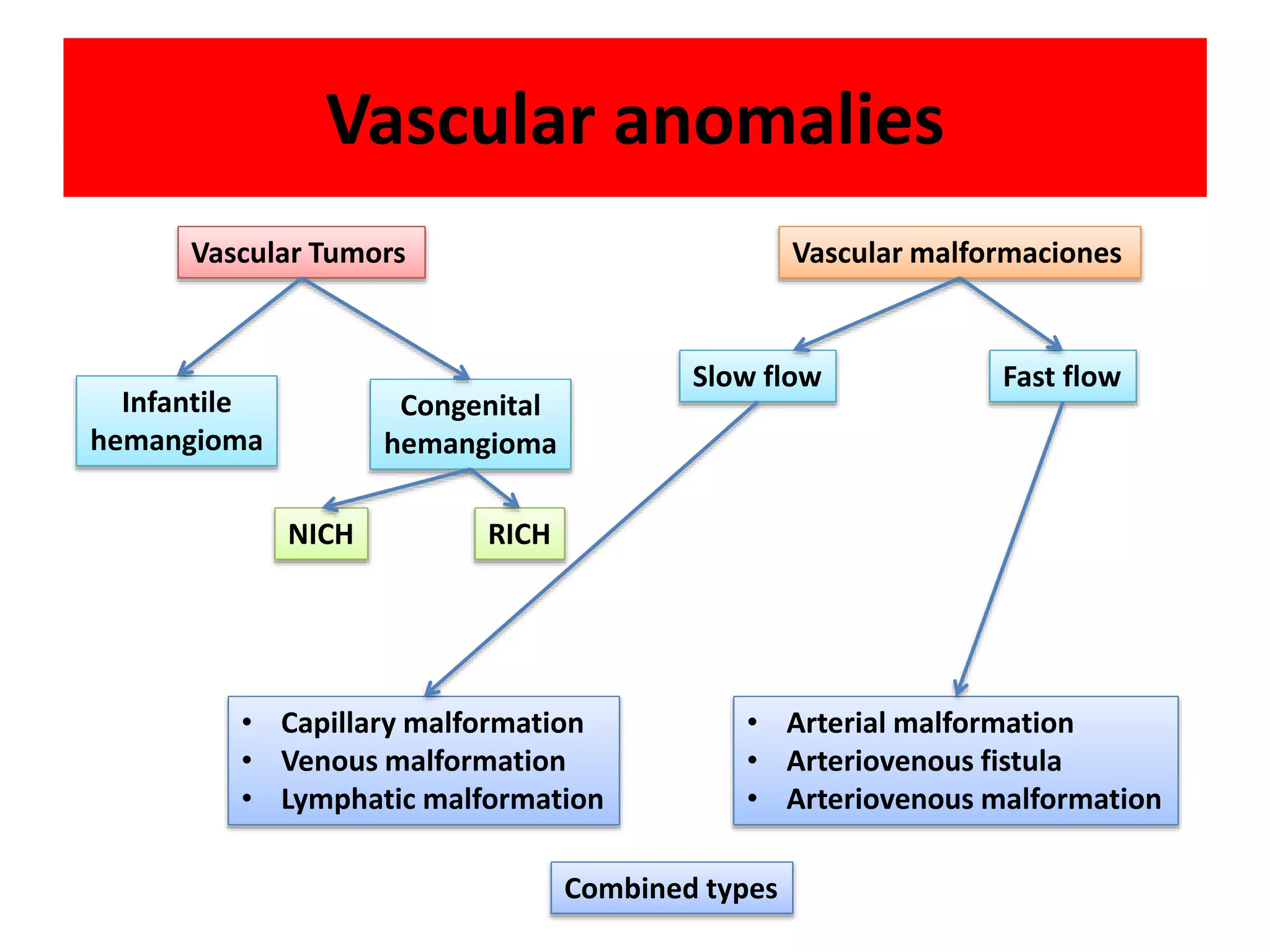
Vascular tumors and malformations are common skin lesions in infants and children. This document discusses several types of vascular tumors: infantile hemangiomas, congenital hemangiomas, kaposiform hemangioendothelioma, and pyogenic granuloma. Infantile hemangiomas are the most common tumor of infancy, appearing as red lesions that grow rapidly during the first year of life and slowly involute over subsequent years. Congenital hemangiomas are fully developed at birth and do not undergo postnatal growth. Kaposiform hemangioendothelioma is a rare but locally aggressive vascular tumor. Pyogenic granuloma is a small red papule that grows rapidly to form a









































































































