Downloaded 210 times
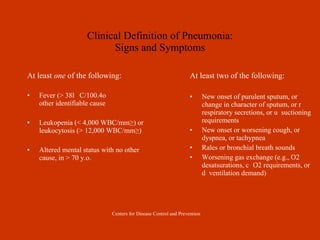

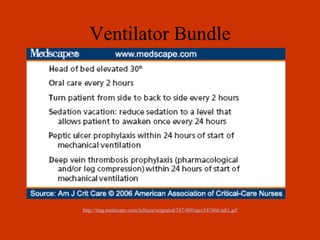
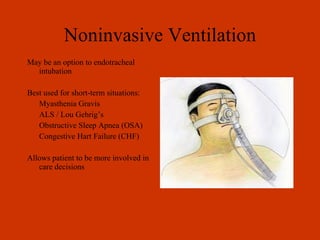

The document discusses the role of respiratory therapists in diagnosing and preventing ventilator-associated pneumonia (VAP). It covers types of healthcare-associated infections including VAP, clinical definitions of pneumonia, diagnostic tests for VAP, treatment approaches, and prevention strategies like oral care, specialized endotracheal tubes, ventilator bundles, and handwashing. Respiratory therapists can reduce VAP rates and costs by following protocols and using evidence-based prevention and treatment methods.










































































