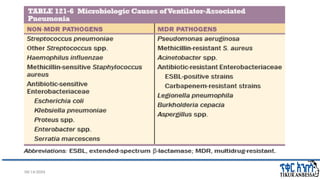
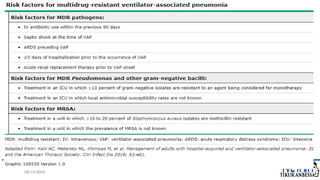
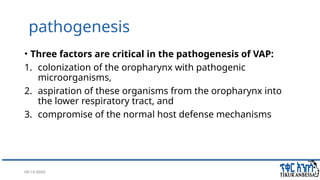
The seminar discusses ventilator-associated pneumonia (VAP), a serious form of pneumonia that occurs in mechanically ventilated patients, highlighting its epidemiology, etiology, clinical presentation, diagnosis, and treatment. VAP is linked to significant mortality rates and requires accurate diagnosis to guide appropriate treatment while avoiding antibiotic resistance. Key factors in its pathogenesis include bacterial colonization, aspiration, and compromised host defenses, with diagnostic approaches favoring invasive sampling to improve specificity.



































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)