Downloaded 678 times
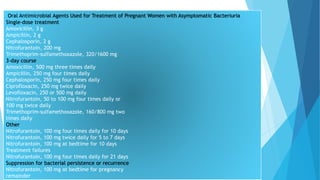





The document discusses urinary tract infections (UTIs) in pregnancy, highlighting that they are the most common bacterial infections in pregnant women, often asymptomatic, but can lead to serious complications such as preterm birth and pyelonephritis. It emphasizes the importance of screening for asymptomatic bacteriuria and provides guidelines for diagnosis and treatment, including specific antibiotics. Additionally, it addresses the implications of HIV during pregnancy, including the risk of vertical transmission and recommended management strategies to reduce transmission risks.

















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





