HOW TO APPROACHURINE EXAMINATION IN PRACTICALS
MBBS – II YEAR PATHOLOGY
Diabetes
Mellitus
Elderly
Polyuria,
Polydipsia,
Polyphagia
Weight loss
Increased
urine volume
Diabetic
Ketoacidosis
Known case
of type 1 DM
Excessive thirst /
frequent
urination /
vomiting
dehydration
Rapid [Kussmaul]
breathing / fruity
odour in breath
Tachycardia
Poor glycemic
control / missing
insulin dose
Nephrotic
Syndrome
Young age
Swelling around
eyes
[periorbital
edema]
Reduced
urine output
Reduced, pale,
frothy urine
Nephritic
Syndrome
Cola coloured
[brown] urine
History of sore
throat / fever /skin
rash
Reduced
urine output
LOOK FOR CLUES IN QUESTION PROVIDED
2.
• URINE POSITIVEFOR SUGAR
DM
• URINE POSITIVE FOR SUGAR
• URINE POSITIVE FOR KETONE BODIES
DKA
• URINE POSITIVE FOR PROTEIN
NEPHROTIC
SYNDROME
• URINE POSITIVE FOR PROTEIN
• URINE POSITIVE FOR BLOOD
NEPHRITIC
SYNDROME
3.
TEST FOR
SUGAR
PROCEDURE
Take 5ml of Benedict’s qualitative reagent in a test tube.
Add 8 drops (or 0.5 ml) of urine.
Heat to boiling for 2 minutes.
Cool in running tap water and look for colour change.
INTERPRETATION
No change of blue colour = Negative
Greenish colour = Traces (< 0.5 g/dl)
Green/cloudy green ppt = + (0.5-1 g/dl)
Yellow ppt = ++ (1-1.5 g/dl)
Orange ppt = +++ (1.5-2 g/dl)
Brick red ppt = ++++ (> 2 g/dl)
CAUSES OF GLYCOSURIA
1. Glycosuria with
hyperglycemia
• Endocrine disorders
Diabetes mellitus
Acromegaly
Cushing’s syndrome
Hyperthyroidism
Hyperadrenocorticism
Pheochromocytoma
• Non-endocrine diseases
Increased intracranial
tension
Liver disorders
Corticosteroids
2. Glycosuria without
hyperglycemia
• Renal glycosuria
Pregnancy
Copper reduction method –
BENEDICT’S TEST Sensitivity of the test is about 200 mg reducing
substance per dl of urine.
Normally a very small amount of glucose
is excreted in urine
(< 500 mg/24 hours or <15 mg/dl)
that cannot be detected by the routine tests.
Presence of detectable amounts of glucose in
urine is called as glucosuria or glycosuria.
Cupric ion is reduced by glucose to cuprous oxide
and a coloured precipitate is formed.
Reducing substances are those compounds which
reduce cupric ions (from copper sulfate in
Benedict’s reagent) in an alkaline solution to cuprous
ions (cuprous oxide).
Such substances may be sugar or non sugar.
1. REDUCING SUGAR: These include: glucose, fructose,
pentose, galactose, lactose, and maltose.
2. NON-REDUCING SUGAR: Sucrose gives negative
result with Benedict’s test since it is a nonreducing
sugar.
3. REDUCING NON-SUGAR: Ascorbic acid, uric acid,
urates, glucuronides, chloroform, formaldehyde,
salicylates, streptomycin, phenol, PAS, homogentisic
acid and creatinine.
4.
HEAT AND ACETICACID
TEST
Coagulati
on of
proteins
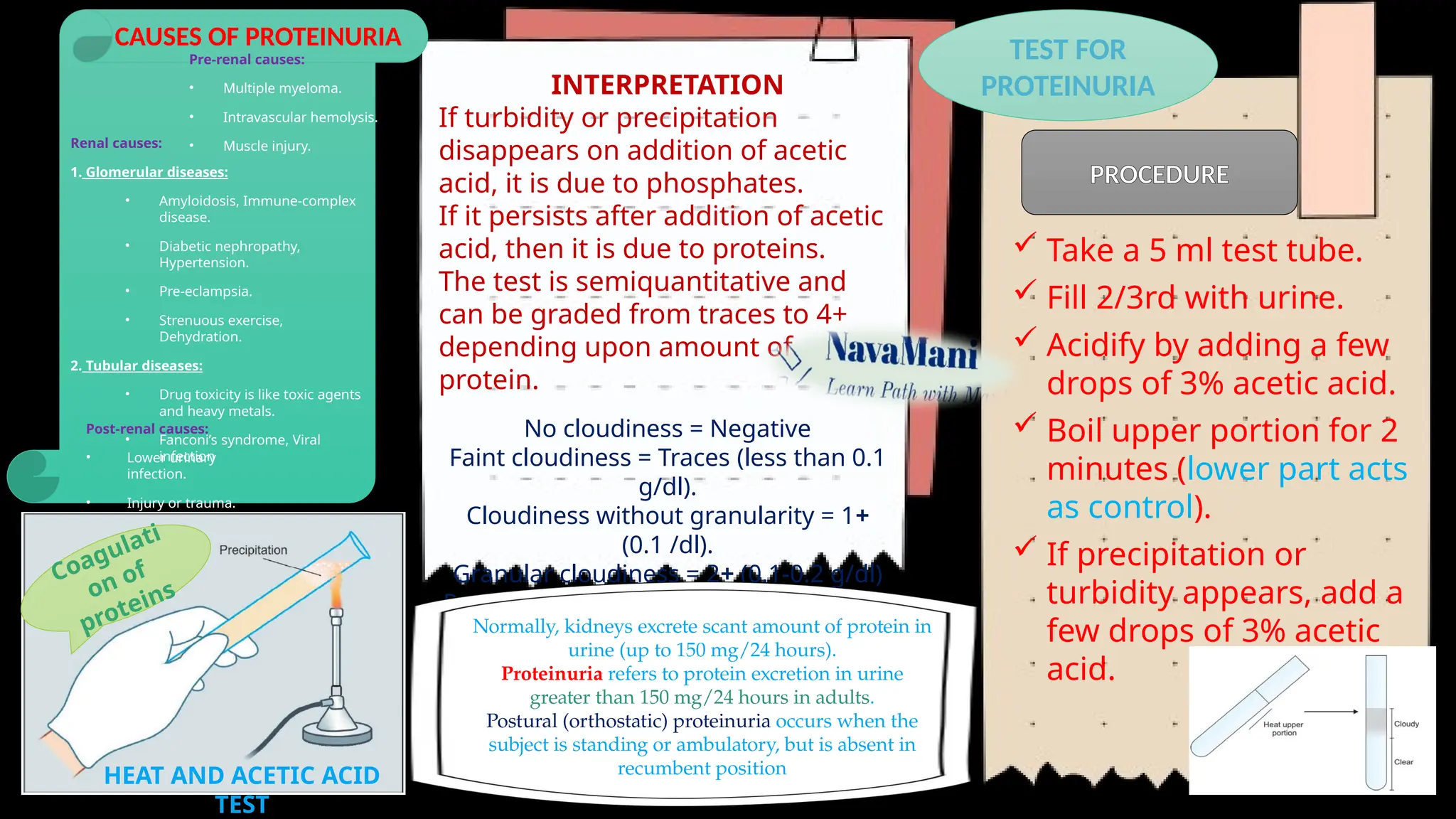
Take a 5 ml test tube.
Fill 2/3rd with urine.
Acidify by adding a few
drops of 3% acetic acid.
Boil upper portion for 2
minutes (lower part acts
as control).
If precipitation or
turbidity appears, add a
few drops of 3% acetic
acid.
INTERPRETATION
If turbidity or precipitation
disappears on addition of acetic
acid, it is due to phosphates.
If it persists after addition of acetic
acid, then it is due to proteins.
The test is semiquantitative and
can be graded from traces to 4+
depending upon amount of
protein.
No cloudiness = Negative
Faint cloudiness = Traces (less than 0.1
g/dl).
Cloudiness without granularity = 1+
(0.1 /dl).
Granular cloudiness = 2+ (0.1-0.2 g/dl)
Precipitation & flocculation = 3+ (0.2-0.4
g/dl).
Thick solid precipitation = 4+ (> 0.5 g/dl).
Normally, kidneys excrete scant amount of protein in
urine (up to 150 mg/24 hours).
Proteinuria refers to protein excretion in urine
greater than 150 mg/24 hours in adults.
Postural (orthostatic) proteinuria occurs when the
subject is standing or ambulatory, but is absent in
recumbent position
PROCEDURE
TEST FOR
PROTEINURIA
CAUSES OF PROTEINURIA
Pre-renal causes:
• Multiple myeloma.
• Intravascular hemolysis.
• Muscle injury.
Renal causes:
1. Glomerular diseases:
• Amyloidosis, Immune-complex
disease.
• Diabetic nephropathy,
Hypertension.
• Pre-eclampsia.
• Strenuous exercise,
Dehydration.
2. Tubular diseases:
• Drug toxicity is like toxic agents
and heavy metals.
• Fanconi’s syndrome, Viral
infection
Post-renal causes:
• Lower urinary
infection.
• Injury or trauma.
5.
TEST FOR
KETONE BODIES
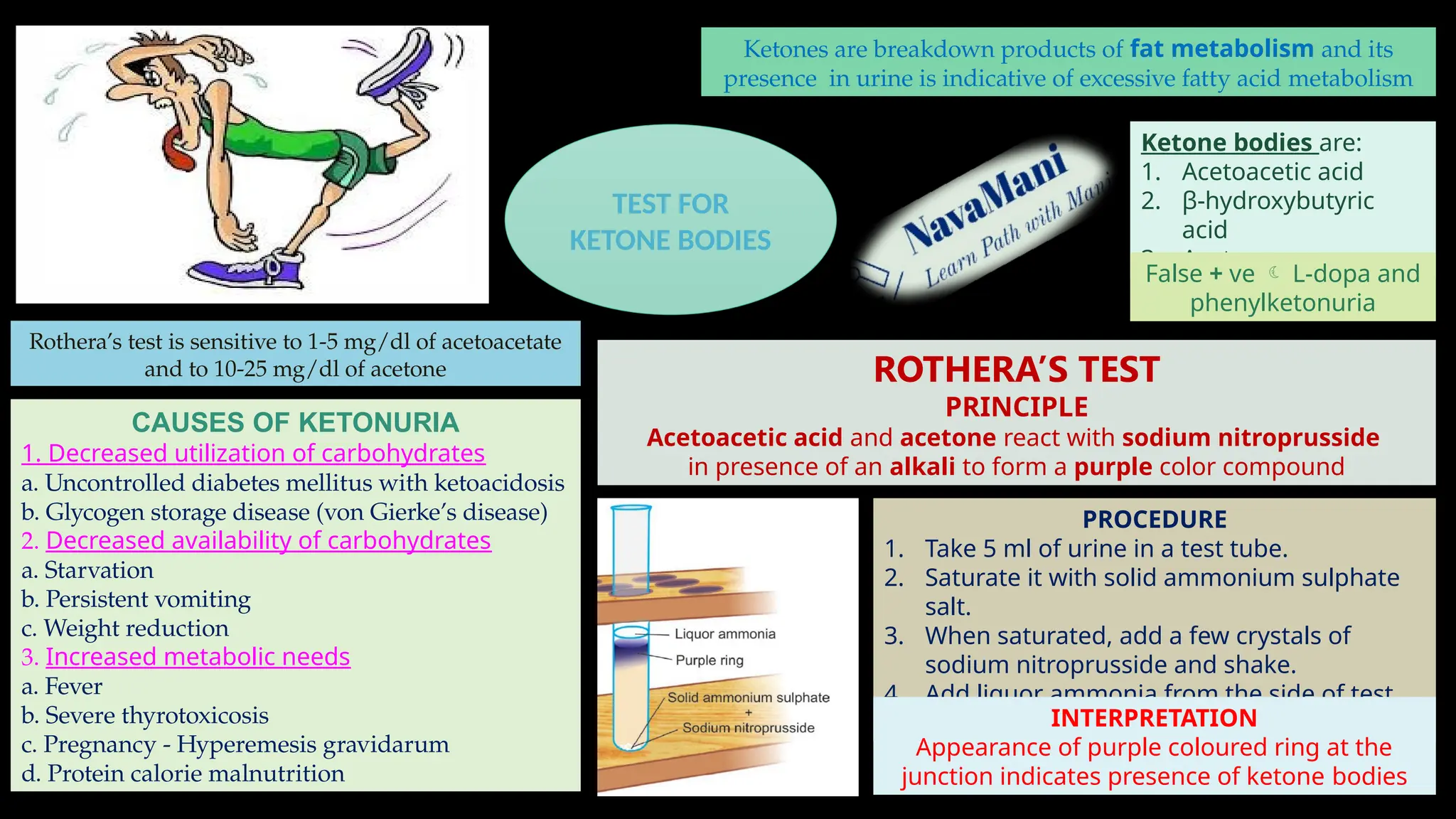
PROCEDURE
1.Take 5 ml of urine in a test tube.
2. Saturate it with solid ammonium sulphate
salt.
3. When saturated, add a few crystals of
sodium nitroprusside and shake.
4. Add liquor ammonia from the side of test
tube. INTERPRETATION
Appearance of purple coloured ring at the
junction indicates presence of ketone bodies
CAUSES OF KETONURIA
1. Decreased utilization of carbohydrates
a. Uncontrolled diabetes mellitus with ketoacidosis
b. Glycogen storage disease (von Gierke’s disease)
2. Decreased availability of carbohydrates
a. Starvation
b. Persistent vomiting
c. Weight reduction
3. Increased metabolic needs
a. Fever
b. Severe thyrotoxicosis
c. Pregnancy - Hyperemesis gravidarum
d. Protein calorie malnutrition
Rothera’s test is sensitive to 1-5 mg/dl of acetoacetate
and to 10-25 mg/dl of acetone ROTHERA’S TEST
PRINCIPLE
Acetoacetic acid and acetone react with sodium nitroprusside
in presence of an alkali to form a purple color compound
Ketone bodies are:
1. Acetoacetic acid
2. β-hydroxybutyric
acid
3. Acetone.
Ketones are breakdown products of fat metabolism and its
presence in urine is indicative of excessive fatty acid metabolism
False + ve L-dopa and
phenylketonuria
6.
TEST FOR
BLOOD
BENZIDINE
TEST
PROCEDURE
1. Makesaturated solution of benzidine in glacial acetic acid.
2. Mix 1 ml of this solution with 1 ml of hydrogen peroxide
(H2O2) in a test tube.
3. Add 2 ml of urine.
INTERPRETATION
Appearance of blue colour indicates presence of blood.
PRINCIPLE
The test depends upon the ability of heme
compounds derived from hemoglobin to
catalyze the oxidation of benzidine by
H2O2
HEMOGLOBINURIA
Presence of free
hemoglobin in urine,
e.g. intravascular
hemolysis.
HEMATURIA
Presence of
abnormal number of
RBCs in urine, e.g.
renal stones, renal
cell carcinoma.
CAUSES OF HEMATURIA
1. Diseases of urinary tract
Glomerular diseases:
Glomerulonephritis,
Berger’s disease,
Lupus nephritis,
Henoch-Schonlein Purpura
Non Glomerular diseases:
Calculus,
Tumor,
Infection,
Tuberculosis,
Pyelonephritis,
Hydronephrosis,
Polycystic kidney disease,
Trauma,
After strenuous physical exercise,
Diseases of prostate (BPH, carcinoma
of prostate).
2. Hematological conditions:
Coagulation disorders,
Sickle cell disease
PRECAUTION
Presence of hypochlorite (bleach) and
microbial peroxidase can cause false
positive results.
Benzidine is carcinogenic.
CAUSES OF FALSE-NEGATIVE TESTS
• Presence of a reducing agent like
ascorbic acid in high concentration.
• Use of formalin as a preservative for
urine
CAUSES OF FALSE-POSITIVE TESTS
• Contamination of urine by
menstrual blood.
• Contamination of urine by oxidizing
agent (e.g. hypochlorite or bleach), or
microbial peroxidase in urinary tract
infection.
![HOW TO APPROACH URINE EXAMINATION IN PRACTICALS
MBBS – II YEAR PATHOLOGY
Diabetes
Mellitus
Elderly
Polyuria,
Polydipsia,
Polyphagia
Weight loss
Increased
urine volume
Diabetic
Ketoacidosis
Known case
of type 1 DM
Excessive thirst /
frequent
urination /
vomiting
dehydration
Rapid [Kussmaul]
breathing / fruity
odour in breath
Tachycardia
Poor glycemic
control / missing
insulin dose
Nephrotic
Syndrome
Young age
Swelling around
eyes
[periorbital
edema]
Reduced
urine output
Reduced, pale,
frothy urine
Nephritic
Syndrome
Cola coloured
[brown] urine
History of sore
throat / fever /skin
rash
Reduced
urine output
LOOK FOR CLUES IN QUESTION PROVIDED](https://image.slidesharecdn.com/urineexamination-250603041018-57bb11d3/75/URINE-EXAMINATION-FOR-PRACTICAL-EXAM-pptx-1-2048.jpg)