Download to read offline
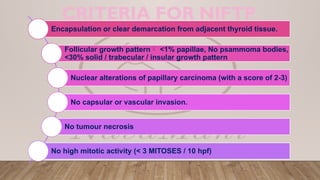
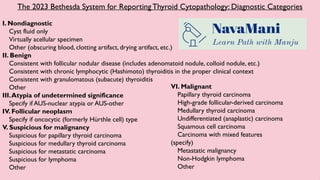


The document outlines diagnostic criteria for thyroid neoplasms based on the 2023 Bethesda System, detailing various categories from nondiagnostic to malignant. It specifies conditions like follicular growth patterns and characteristics of atypia or malignancy, including specific types of thyroid carcinoma. It emphasizes the importance of clear demarcation from adjacent tissues and the absence of invasive features in benign conditions.



































































