The document provides an overview of the anatomy and functions of the urinary system. It describes the major components including the kidneys, ureters, urinary bladder, and urethra. The kidneys filter waste from the blood and produce urine, which travels through the ureters to the bladder. The bladder stores urine until urination, when it is expelled through the urethra. Key structures like the nephrons and vasculature are also summarized.
If you want to help or donate please donate at my paypal:
dyokimura@gmail.com
SUPPORT ME:
https://www.buymeacoffee.com/dyokimura6
CHECK MY GAMING CHANNEL:
https://www.youtube.com/channel/UCoKOObshfyyxhVkw1VjyQNA
Note on assessment of renal or urinary systemBabitha Devu
A guide to help the students review themselves about the A & P of the urinary system. it also helps in collecting history and appraise the client suffering from various urinary tract disorders or diseases.
Urinary system
a) Anatomy and physiology of urinary system
b) Formation of urine
c) Renin Angiotensin system – Juxtaglomerular apparatus - acid base Balance
d) Clearance tests and micturition
6. ANATOMY OF THE KIDNEY, URETER & POSTERIOR.pdfmarkmuiruri581
Anatomy of Urinary System
Urinary System Organs
Kidneys (2)
Ureters (2)
Urinary bladder
Urethra
Kidney Functions
Control blood volume and composition.
Filter blood plasma, eliminate wastes.
Regulate blood volume, pressure, and fluid osmolarity.
Secrete renin and erythropoietin (EPO).
Regulate PCO2, acid-base balance.
Synthesize calcitriol (Vitamin D).
Detoxify free radicals and drugs.
Perform gluconeogenesis.
Kidney Anatomy
Renal Fascia: Attaches to the abdominal wall.
Adipose Capsule: Provides fat cushioning for the kidney.
Renal Capsule: Fibrous sac that protects from trauma and infection.
Renal Sinus: Contains blood vessels, lymphatics, nerves, and urine-collecting structures.
Renal Parenchyma:
Outer Cortex
Inner Medulla
Renal Pyramids: Extensions of cortex dividing medulla.
Renal Columns: Connect cortex and medulla.
Renal Pelvis: Collects urine from pyramids.
Ureter: Carries urine to the bladder.
Remember, the kidneys play a crucial role in maintaining homeostasis by regulating fluid balance, electrolytes, and waste elimination. Ureter Anatomy
Overview
The ureters are bilateral, muscular, tubular structures responsible for transporting urine from the kidneys to the urinary bladder for storage and eventual excretion.
After blood filtration in the kidneys, the filtrate undergoes reabsorption and exudation along the convoluted tubules.
The urine then passes through the collecting tubules and enters the collecting ducts.
From the collecting ducts, it flows through the calyces into the renal pelvis, marking the beginning of the ureters.
Histology of Ureter
The lumen of each ureter is lined by a mucosal layer of urothelium (transitional epithelium).
The ureteral wall contains two muscular layers:
Longitudinal layer
Circular layer
In the lower segment of the ureters, an additional longitudinal layer is found proximal to the bladder.
Urine is propelled along the ureters by peristaltic motions initiated by pacemaker cells in the proximal renal pelvis.
Relations
Both ureters pass inferiorly over the abdominal surface of the psoas major muscle.
The right ureter travels posterior to the duodenum and is crossed by branches of the superior mesenteric vessels.
The left ureter is also posterior to the psoas major and is crossed by branches of the inferior mesenteric vessels.
Posterior Abdominal Wall
Construction
Bony: Extends from the 12th rib above to the pelvic brim below.
Muscular part: Composed of muscles and fasciae.
Fasciae: Provides stability and support for retroperitoneal organs, vessels, and nerves.
Remember, understanding the anatomy of the ureter and posterior abdominal wall is essential for clinical pracPosterior Abdominal Wall
Construction
Bony: Extends from the 12th rib above to the pelvic brim below.
Muscular part: Composed of muscles and fasciae.
Fasciae: Provides stability and support for retroperitoneal organs, vessels, and nerves.
Muscles of Posterior Abdominal Wall
Psoas Major:
Origin: Continuously attached from T12 (lower border) to L5
these slides are prepared to understand Urinary system IN EASY WAY Important links- NOTES- https://mynursingstudents.blogspot.com/ youtube channel https://www.youtube.com/c/MYSTUDENTSU... CHANEL PLAYLIST- ANATOMY AND PHYSIOLOGY-https://www.youtube.com/playlist?list=PL93S13oM2gAPM3VTGVUXIeswKJ3XGaD2p COMMUNITY HEALTH NURSING- https://www.youtube.com/playlist?list=PL93S13oM2gAPyslPNdIJoVjiXEDTVEDzs CHILD HEALTH NURSING- https://www.youtube.com/playlist?list=PL93S13oM2gANcslmv0DXg6BWmWN359Gvg FIRST AID- https://www.youtube.com/playlist?list=PL93S13oM2gAMvGqeqH2ZTklzFAZhOrvgP HCM- https://www.youtube.com/playlist?list=PL93S13oM2gAM7mZ1vZhQBHWbdLnLb-cH9 FUNDAMENTALS OF NURSING- https://www.youtube.com/playlist?list=PL93S13oM2gAPFxu78NDLpGPaxEmK1fTao COMMUNICABLE DISEASES- https://www.youtube.com/playlist?list=PL93S13oM2gAOWo4IwNjLU_LCuhRN0ZLeb ENVIRONMENTAL HEALTH- https://www.youtube.com/playlist?list=PL93S13oM2gAPkI6LvfS8Zu1nm6mZi9FK6 MSN- https://www.youtube.com/playlist?list=PL93S13oM2gAOdyoHnDLAoR_o8M6ccqYBm HINDI ONLY- https://www.youtube.com/playlist?list=PL93S13oM2gAN4L-FJ3s_IEXgZCijGUA1A ENGLISH ONLY- https://www.youtube.com/playlist?list=PL93S13oM2gAMYv2a1hFcq4W1nBjTnRkHP facebook profile- https://www.facebook.com/suresh.kr.lrhs/ FACEBOOK PAGE- https://www.facebook.com/My-Student-S... facebook group NURSING NOTES- https://www.facebook.com/groups/24139... FOR MAKING EASY NOTES YOU CAN ALSO VISIT MY BLOG – BLOGGER- https://mynursingstudents.blogspot.com/ Instagram- https://www.instagram.com/mystudentsu... Twitter- https://twitter.com/student_system?s=08
#Nephrons, #kidney, #urine, #BORN,#ASSESSMENT, #APPEARENCE,#PULSE,#GRIMACE,#REFLEX,#RESPIRATION,#RESUSCITATION,#NEWBORN,#BABY,#VIRGINIA, #APGAR, #OXYGEN,#CYANOSIS,#OPTICNERVE, #SARACHNA,#MYSTUDENTSUPPORTSYSTEM, #rashes,#nursingclasses, #communityhealthnursing,#ANM, #GNM, #BSCNURING,#NURSINGSTUDENTS, #WHO,#NURSINGINSTITUTION,#COLLEGEOFNURSING,#nursingofficer,#COMMUNITYHEALTHOFFICER
If you want to help or donate please donate at my paypal:
dyokimura@gmail.com
SUPPORT ME:
https://www.buymeacoffee.com/dyokimura6
CHECK MY GAMING CHANNEL:
https://www.youtube.com/channel/UCoKOObshfyyxhVkw1VjyQNA
Note on assessment of renal or urinary systemBabitha Devu
A guide to help the students review themselves about the A & P of the urinary system. it also helps in collecting history and appraise the client suffering from various urinary tract disorders or diseases.
Urinary system
a) Anatomy and physiology of urinary system
b) Formation of urine
c) Renin Angiotensin system – Juxtaglomerular apparatus - acid base Balance
d) Clearance tests and micturition
6. ANATOMY OF THE KIDNEY, URETER & POSTERIOR.pdfmarkmuiruri581
Anatomy of Urinary System
Urinary System Organs
Kidneys (2)
Ureters (2)
Urinary bladder
Urethra
Kidney Functions
Control blood volume and composition.
Filter blood plasma, eliminate wastes.
Regulate blood volume, pressure, and fluid osmolarity.
Secrete renin and erythropoietin (EPO).
Regulate PCO2, acid-base balance.
Synthesize calcitriol (Vitamin D).
Detoxify free radicals and drugs.
Perform gluconeogenesis.
Kidney Anatomy
Renal Fascia: Attaches to the abdominal wall.
Adipose Capsule: Provides fat cushioning for the kidney.
Renal Capsule: Fibrous sac that protects from trauma and infection.
Renal Sinus: Contains blood vessels, lymphatics, nerves, and urine-collecting structures.
Renal Parenchyma:
Outer Cortex
Inner Medulla
Renal Pyramids: Extensions of cortex dividing medulla.
Renal Columns: Connect cortex and medulla.
Renal Pelvis: Collects urine from pyramids.
Ureter: Carries urine to the bladder.
Remember, the kidneys play a crucial role in maintaining homeostasis by regulating fluid balance, electrolytes, and waste elimination. Ureter Anatomy
Overview
The ureters are bilateral, muscular, tubular structures responsible for transporting urine from the kidneys to the urinary bladder for storage and eventual excretion.
After blood filtration in the kidneys, the filtrate undergoes reabsorption and exudation along the convoluted tubules.
The urine then passes through the collecting tubules and enters the collecting ducts.
From the collecting ducts, it flows through the calyces into the renal pelvis, marking the beginning of the ureters.
Histology of Ureter
The lumen of each ureter is lined by a mucosal layer of urothelium (transitional epithelium).
The ureteral wall contains two muscular layers:
Longitudinal layer
Circular layer
In the lower segment of the ureters, an additional longitudinal layer is found proximal to the bladder.
Urine is propelled along the ureters by peristaltic motions initiated by pacemaker cells in the proximal renal pelvis.
Relations
Both ureters pass inferiorly over the abdominal surface of the psoas major muscle.
The right ureter travels posterior to the duodenum and is crossed by branches of the superior mesenteric vessels.
The left ureter is also posterior to the psoas major and is crossed by branches of the inferior mesenteric vessels.
Posterior Abdominal Wall
Construction
Bony: Extends from the 12th rib above to the pelvic brim below.
Muscular part: Composed of muscles and fasciae.
Fasciae: Provides stability and support for retroperitoneal organs, vessels, and nerves.
Remember, understanding the anatomy of the ureter and posterior abdominal wall is essential for clinical pracPosterior Abdominal Wall
Construction
Bony: Extends from the 12th rib above to the pelvic brim below.
Muscular part: Composed of muscles and fasciae.
Fasciae: Provides stability and support for retroperitoneal organs, vessels, and nerves.
Muscles of Posterior Abdominal Wall
Psoas Major:
Origin: Continuously attached from T12 (lower border) to L5
these slides are prepared to understand Urinary system IN EASY WAY Important links- NOTES- https://mynursingstudents.blogspot.com/ youtube channel https://www.youtube.com/c/MYSTUDENTSU... CHANEL PLAYLIST- ANATOMY AND PHYSIOLOGY-https://www.youtube.com/playlist?list=PL93S13oM2gAPM3VTGVUXIeswKJ3XGaD2p COMMUNITY HEALTH NURSING- https://www.youtube.com/playlist?list=PL93S13oM2gAPyslPNdIJoVjiXEDTVEDzs CHILD HEALTH NURSING- https://www.youtube.com/playlist?list=PL93S13oM2gANcslmv0DXg6BWmWN359Gvg FIRST AID- https://www.youtube.com/playlist?list=PL93S13oM2gAMvGqeqH2ZTklzFAZhOrvgP HCM- https://www.youtube.com/playlist?list=PL93S13oM2gAM7mZ1vZhQBHWbdLnLb-cH9 FUNDAMENTALS OF NURSING- https://www.youtube.com/playlist?list=PL93S13oM2gAPFxu78NDLpGPaxEmK1fTao COMMUNICABLE DISEASES- https://www.youtube.com/playlist?list=PL93S13oM2gAOWo4IwNjLU_LCuhRN0ZLeb ENVIRONMENTAL HEALTH- https://www.youtube.com/playlist?list=PL93S13oM2gAPkI6LvfS8Zu1nm6mZi9FK6 MSN- https://www.youtube.com/playlist?list=PL93S13oM2gAOdyoHnDLAoR_o8M6ccqYBm HINDI ONLY- https://www.youtube.com/playlist?list=PL93S13oM2gAN4L-FJ3s_IEXgZCijGUA1A ENGLISH ONLY- https://www.youtube.com/playlist?list=PL93S13oM2gAMYv2a1hFcq4W1nBjTnRkHP facebook profile- https://www.facebook.com/suresh.kr.lrhs/ FACEBOOK PAGE- https://www.facebook.com/My-Student-S... facebook group NURSING NOTES- https://www.facebook.com/groups/24139... FOR MAKING EASY NOTES YOU CAN ALSO VISIT MY BLOG – BLOGGER- https://mynursingstudents.blogspot.com/ Instagram- https://www.instagram.com/mystudentsu... Twitter- https://twitter.com/student_system?s=08
#Nephrons, #kidney, #urine, #BORN,#ASSESSMENT, #APPEARENCE,#PULSE,#GRIMACE,#REFLEX,#RESPIRATION,#RESUSCITATION,#NEWBORN,#BABY,#VIRGINIA, #APGAR, #OXYGEN,#CYANOSIS,#OPTICNERVE, #SARACHNA,#MYSTUDENTSUPPORTSYSTEM, #rashes,#nursingclasses, #communityhealthnursing,#ANM, #GNM, #BSCNURING,#NURSINGSTUDENTS, #WHO,#NURSINGINSTITUTION,#COLLEGEOFNURSING,#nursingofficer,#COMMUNITYHEALTHOFFICER
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stockrebeccabio
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stock
Telegram: bmksupplier
signal: +85264872720
threema: TUD4A6YC
You can contact me on Telegram or Threema
Communicate promptly and reply
Free of customs clearance, Double Clearance 100% pass delivery to USA, Canada, Spain, Germany, Netherland, Poland, Italy, Sweden, UK, Czech Republic, Australia, Mexico, Russia, Ukraine, Kazakhstan.Door to door service
Hot Selling Organic intermediates
Prix Galien International 2024 Forum ProgramLevi Shapiro
June 20, 2024, Prix Galien International and Jerusalem Ethics Forum in ROME. Detailed agenda including panels:
- ADVANCES IN CARDIOLOGY: A NEW PARADIGM IS COMING
- WOMEN’S HEALTH: FERTILITY PRESERVATION
- WHAT’S NEW IN THE TREATMENT OF INFECTIOUS,
ONCOLOGICAL AND INFLAMMATORY SKIN DISEASES?
- ARTIFICIAL INTELLIGENCE AND ETHICS
- GENE THERAPY
- BEYOND BORDERS: GLOBAL INITIATIVES FOR DEMOCRATIZING LIFE SCIENCE TECHNOLOGIES AND PROMOTING ACCESS TO HEALTHCARE
- ETHICAL CHALLENGES IN LIFE SCIENCES
- Prix Galien International Awards Ceremony
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
MANAGEMENT OF ATRIOVENTRICULAR CONDUCTION BLOCK.pdfJim Jacob Roy
Cardiac conduction defects can occur due to various causes.
Atrioventricular conduction blocks ( AV blocks ) are classified into 3 types.
This document describes the acute management of AV block.
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
Anti ulcer drugs and their Advance pharmacology ||
Anti-ulcer drugs are medications used to prevent and treat ulcers in the stomach and upper part of the small intestine (duodenal ulcers). These ulcers are often caused by an imbalance between stomach acid and the mucosal lining, which protects the stomach lining.
||Scope: Overview of various classes of anti-ulcer drugs, their mechanisms of action, indications, side effects, and clinical considerations.
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...GL Anaacs
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
3. Objectives
At end of this session students able to know:
Describe the external and internal gross anatomical features of
the kidneys
Outline the path of blood flow through the kidneys
Describe the structure of renal corpuscles and renal tubules
Describe the anatomy of the ureters, urinary bladder, and
urethra.
Understand the innervation and vasculature of the urinary
organs
3
5. Functions of urinary system
Filtrations of blood, allowing
toxins, metabolic wastes, and
excess ions to leave the body
in urine.
Regulate volume and chemical
makeup of the blood.
Maintain the proper balance
between water and salts, and
acids and bases.
Production hormones-
calcitriol and erythropoietin.
5
6. Kidneys
Paired kidneys are reddish and
bean–shaped organs
Located just above the waist
between the peritoneum and the
posterior wall of the abdomen
(called retroperitoneal organ).
Kidneys are located between the
levels of the last thoracic and
third lumbar vertebrae (T12- L3).
They are partially protected by
ribs 11 and 12.
6
8. External Anatomy of the Kidneys
A typical adult kidney is :
– 10–12 cm long
– 5–7 cm wide
– 3 cm thick
– Has a mass of 135–150 g
Right kidney is slightly
lower than the left .
– Because the liver occupies
considerable space on the
right side superior to the
kidney
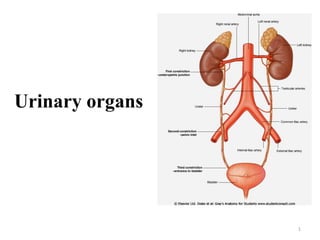
Anterior view of urinary system
8
9. Structure of the kidney
Each kidney has:
Anterior and posterior
surface
Medial borders (concave)
Lateral borders (convex)
Superior and inferior
poles.
On the medial side of each
kidney is a small area called
the hilum.
Ureters, renal blood vessels,
lymphatics, and nerves enter
and exit at the hilum.
9
10. Kidneys
The concave medial border of each kidney faces the vertebral
column
Near the center of the concave border is an indentation called the
renal hilum
Through which the ureter emerges from the kidney along with
blood vessels, lymphatic vessels, and nerves.
10
11. Three layers of tissue surround each kidney
From deep to superficial
– Renal capsule
– Adipose capsule
– Renal fascia
11
12. 12
1. Renal capsule
– Deep layer
– It is a smooth, transparent sheet of dense irregular connective tissue
that is continuous with the outer coat of the ureter.
– It serves as a barrier against trauma and helps maintain the shape of
the kidney.
– Inner layer of fibrous capsule that prevents kidney infection.
2. Adipose capsule
– Middle layer
– Fatty mass that cushions the kidney and helps attach it to the body
wall
– It also protects the kidney from trauma and holds it firmly in place
within the abdominal cavity.
3. Renal fascia
– Outer layer of dense fibrous connective tissue.
– That anchors the kidney to the surrounding structures and to the
abdominal wall.
13. Internal Anatomy of Kidneys
Kidney is divided into two parts
1. An outer renal cortex:
superficial, light red region
2. An inner medulla: a deep,
darker reddish-brown inner
region
Medulla- consists of a number
of cone shaped renal pyramids.
The base of each pyramid is
located at the boundary b/n the
cortex & the medulla.
Renal papillae- are tips of the
pyramids that projects into the
renal sinus. 13
14. Renal cortex is the
smooth-textured area.
Extending from the renal
capsule to the bases of the
renal pyramids and into
the spaces between them.
Extensions of the cortex
called renal columns
project b/n the pyramids.
14
Internal Anatomy of Kidneys
15. Microscopic Structure of the kidney
NEPHRON
Nephron is the structural and
functional unit of the kidney.
Each kidney contains
approximately 1 million
nephrons.
Filtrate (filtered fluid) formed
by the nephrons drains into
large papillary ducts.
– Which extend through the
renal papillae of the pyramids.
The papillary ducts drain into
cuplike structures called minor
and major calyces.
15
16. Internal Anatomy…
Minor calyces- are funnel
shaped structure that
surround the renal papillae.
Major calyces- larger
funnels formed from the
joining together of minor
calyces.
There are 8-20 minor
calyces & 2 or 3 major
calyces per kidney.
Renal pelvis- a single large
cavity that delivers urine from
major calyx to a small tube the
ureters. 16
18. 18
Renal tubules
Nephrons consists of :-
- Bowman’s capsule
- A proximal convoluted tubule
- A loop of Henle
- A distal convoluted tube
- Collecting duct w/c carrier the urine from the cortex to the
calyces
The bowman’s capsule & both convoluted tubules are in the renal
cortex.
The collecting tubules & part of the loops of Henle enter the renal
medulla → Renal papilla → Minor calyx → Major calyx →
Renal pelvis Ureter
20. Blood and Nerve Supply of the Kidneys
Although the kidneys constitute less than 0.5% of total body
mass.
They receive 20–25% of the resting cardiac output via the
right and left renal arteries.
In adults, renal blood flow, the blood flow through both
kidneys, is about 1200 mL per minute.
20
21. Vasculature of kidney
Renal artery: supplies each kidney.
Right renal artery is longer and passes posterior to the
inferior vena cava.
Accessory renal arteries or extrahilar arteries are common.
21
22. Renal blood vessels
Arterial blood enters the kidney through the renal artery-
Segmental arteries - interlobar arteries -the actuate arteries
–interlobular arteries-afferent arterioles.
Deliver blood into glomeruli capillary w/c produce a blood
filtrate that enters the urinary tubules.
Veins drainage
Efferent arterioles – peritubular capillaries – interlobular
veins – arcuate veins – interlobar veins - renal veins –
inferior vena cava.
22
25. Ureters
Ureters - a muscular tubular
organ 25cm long each
The renal pelvis becomes
continuous with the ureter at
the uretero pelvic junction.
Extends from the renal pelvis
to the bladder.
Conduct urine to the urinary
bladder.
It is retroperitoneal organ. 25
26. Ureters
Each of the two ureters transports
urine from the renal pelvis of one
kidney to the urinary bladder.
Peristaltic contractions of the
muscular walls of the ureters push
urine toward the urinary bladder.
Hydrostatic pressure and gravity
also contribute.
Transitional epithelium is able to
stretch a marked advantage for any
organ that must accommodate a
variable volume of fluid.
26
27. Ureteric constriction
At three points along their course
the ureters are constricted:
I. At the uretero pelvic junction
II. Where the ureters cross the
common iliac vessels at the
pelvic brim
III. Where the ureters enter the
wall of the bladder.
27
28. Vasculature of Ureters
Arterial supply to the pelvic
parts of the ureters is variable.
– Common iliac, internal iliac,
and ovarian arteries.
The most constant arteries
supplying the terminal parts of
the ureter in females are
branches of the uterine
arteries.
Venous drainage from the
pelvic parts of the ureters
generally parallels the arterial
supply.
28
29. Urinary tract stones (calculi)
Occurrence of stone or calculi in ureter.
Occur more frequently in men than in women.
Most common in people aged between 20 and 60 years.
The typical presentation is a patient with pain that radiates from
the loin region into the groin, and even into the scrotum or labia
majora.
Blood in the urine (hematuria) may also be noticed.
The complications of urinary tract stones include infection,
urinary obstruction, and renal failure.
29
30. Urinary Bladder
A hollow, distensible muscular
organ.
Situated in the pelvic cavity
posterior to the pubic symphysis.
It is characterized by its
distensibility.
Bladder is a temporary reservoir
for urine and it contracts to
eliminate urine.
Varies in size, shape, position, and
relationships according to its
content, and the state of
neighboring viscera.
30
31. Position
In adults:
– Empty bladder lies in pelvis
minor posterior and slightly
superior to pubic bones.
– When filled ascends to
pelvic major and abdomen.
In infants: found in abdomen
– Enters pelvic major at about
6 years of age and pelvic
minor at puberty.
In males, it is directly anterior
to the rectum.
In females, it is anterior to the
vagina and inferior to the
uterus.
31
Urinary Bladder…….
32. Folds of the peritoneum hold
the urinary bladder in
position.
When slightly distended due
to the accumulation of urine,
the urinary bladder is
spherical.
When it is empty, it collapses.
Urinary bladder capacity
averages 700–800 mL.
Capacities in the adult male
vary from 120 – 320ml.
Micturition usually occurring
at 280 mL
When the bladder is filled it
contains about 500 mL 32
Urinary Bladder
33. Anatomy and Histology of the Urinary Bladder
In the floor of the urinary bladder is a small triangular area called
trigone.
The opening of the two ureters and the urethra mark a smooth
surface triangular area is called trigone on the bladder floor.
The opening into the urethra, the internal urethral orifice, lies in
the anterior corner.
33
34. Arterial supply
Branches of internal iliac arteries
Superior vesical artery: supply anterosuperior parts
Inferior vesical artery and Vaginal artery: supply fundus
(posterioinferior) in male and female, respectively
Venous drainage
Correspond to arteries and drain into internal iliac vein.
Lymphatic drainage
Superior part: to external iliac lymph nodes
Inferior part: to internal iliac lymph nodes
34
Vasculature of Bladder
35. CLINICAL CONNECTION | Urinary Incontinence
A lack of voluntary control over micturition is called urinary
incontinence.
In infants and children under 2–3 years old, incontinence is
normal because neurons to the external urethral sphincter muscle
are not completely developed.
Voiding occurs whenever the urinary bladder is sufficiently
distended to stimulate the micturition reflex.
Urinary incontinence also occurs in adults.
There are four types of urinary incontinence—
– Stress
– Urge
– Overflow
– Functional
35
36. Urethra
Tubular, conveys urine from
urinary bladder to outside.
Its wall contains mucus
secreting urethral glands.
Tube extend from internal
urethral orifice to exterior.
Passage way for discharging
urine (and semen in male).
Consists of two muscular
sphincters:
– Internal urethral sphincter –
formed from the detrusor
muscle of bladder (smooth
muscle)
– External urethral sphincter –
voluntary skeletal muscle. 36
37. Females urethra
The urethra lies directly posterior to the pubic symphysis.
4cm long, empties urine through urethral orifice into the
vestibule b/n the labia minora.
Positioned immediately anterior to the vaginal orifice, and 2.5cm
posterior to the clitoris.
Opening of the urethra to the exterior, external urethral orifice
– Located between the clitoris and the vaginal opening
37
38. Male Urethra
It is about 18-20 cm long.
Extends from the internal urethral orifice in the bladder to the
external meatus.
Located at the tip of the glans penis in males.
Serves both as urinary and reproductive systems
Conveys urine from urinary bladder to the exterior.
Also provides an exit for semen (sperm + seminal fluid).
38
39. 39
Parts of Male Urethra
S-shaped because of the shape of penis.
40. Parts of Male Urethra
Has three parts:
1. Prostatic Part-
– Descends through the prostate
gland.
– Varies in diameter and length.
– Depending on whether the
bladder is filling.
– This is 3-4 cm long
– The widest & most dilatable
part of the urethra
– Receives drainage from bladder,
prostate, and ejaculatory ducts.
40
41. Parts of Male Urethra
2. Membranous Part
It is the shortest part (1-2cm) and least dilatable part.
Thinnest and narrowest (except external urethral orifice) .
Posterolateral to it on each side is bulbourethral gland and duct.
41
42. Parts of Male Urethra
3. Spongy part
Is the part with in the penis.
The longest part 10 to 16 cm long.
Lies in the corpus spongiosum of penis.
Extends from bulbs body to external urethral orifice.
Expanded in bulb and in glans penis.
42