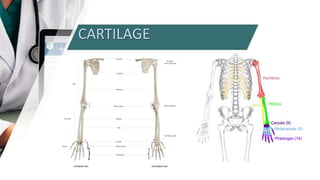
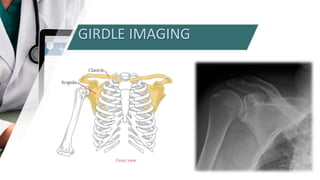
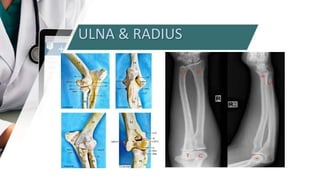
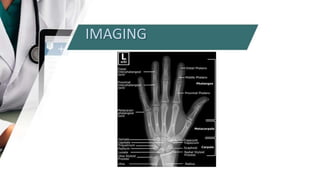
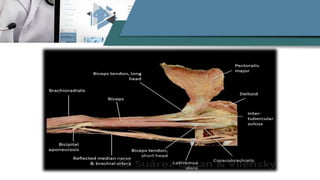
The upper limb consists of the arm, forearm, and hand. The arm has one bone, the humerus. The forearm has two bones, the radius and ulna. The hand has 27 bones grouped into carpals, metacarpals, and phalanges. The shoulder girdle connects the upper limbs to the axial skeleton and consists of the clavicle and scapula. The bones of the upper limb allow for mobility and manipulation and are connected by muscles that act on the joints of the shoulder, elbow, wrist, and fingers.