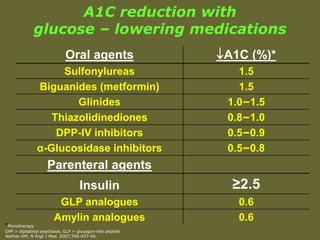
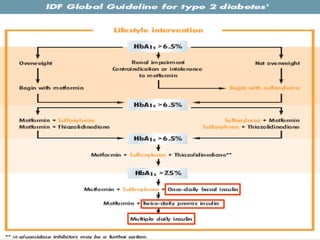
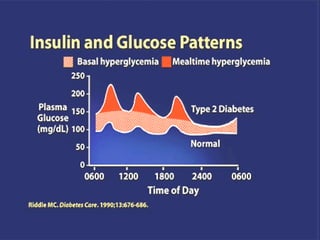
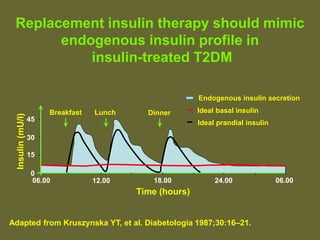
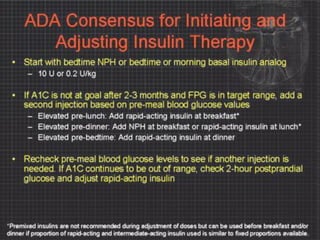
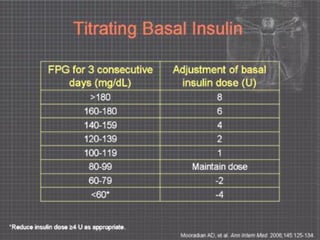
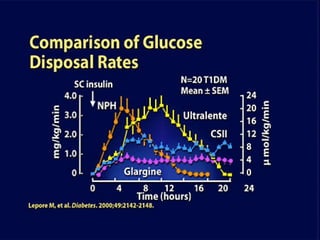
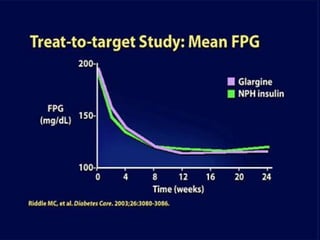
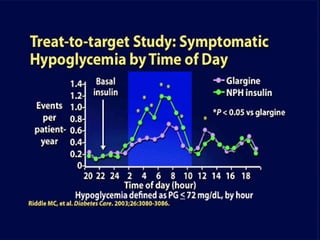
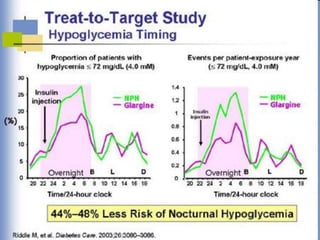
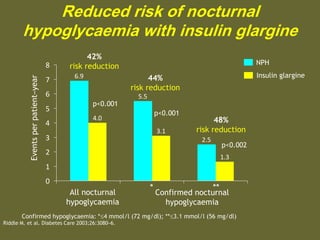
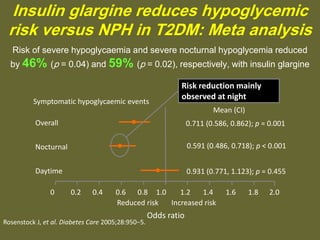
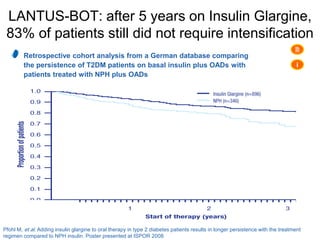
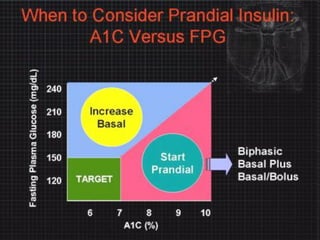
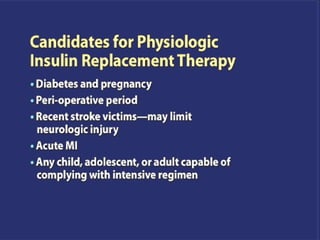
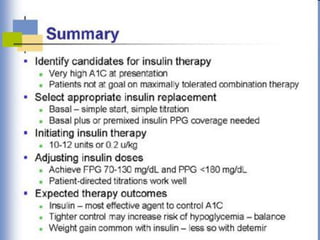
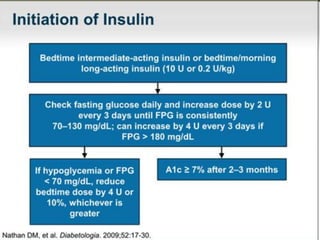
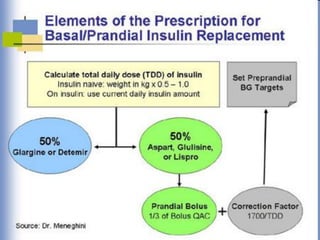
This document discusses challenges and solutions for insulin therapy in primary care. It begins by reviewing different glucose-lowering medications and their typical A1C reduction, with insulin providing the greatest reduction of at least 2.5%. The document then recommends starting insulin first for patients with A1C over 10%, fasting blood sugar over 250 mg/dl, or random blood sugar consistently over 300 mg/dl. It advocates that replacement insulin therapy should mimic the body's natural insulin profile. The rest of the document discusses the benefits of basal insulin, particularly insulin glargine, in reducing risks of hypoglycemia and improving 24-hour glucose control compared to NPH insulin. It emphasizes that education for patients on insulin therapy is important.