Tuberculosis
Tuberculosis (TB) iscaused by a bacterium called Mycobacterium tuberculosis. The bacteria
usually attack the lungs, but TB bacteria can attack any part of the body such as the kidney,
spine, and brain.The name mycobacterium is derived from the word “mold” meaning fungus like
bacterium.
Causative agent:
● Straight or slightly curved thin rod-shaped bacilli.
● Non-sporing, non-motile, non-capsulated bacteria.
● Acid-fast bacilli, neither gram +ve nor gram –ve.
● During acid-fast stains, they appear bright red to intense purple with a green/blue
background.
● The high content of mycolic acid (50 to 60 %).
● The cell wall is rich in lipids and waxes.
● Solid medium for growth - Lowenstein Jensen medium
● Liquid medium - Dubos medium
Pathogenesis:
The pathogenesis is based on reactions of the cellular immune system with TB antigens.
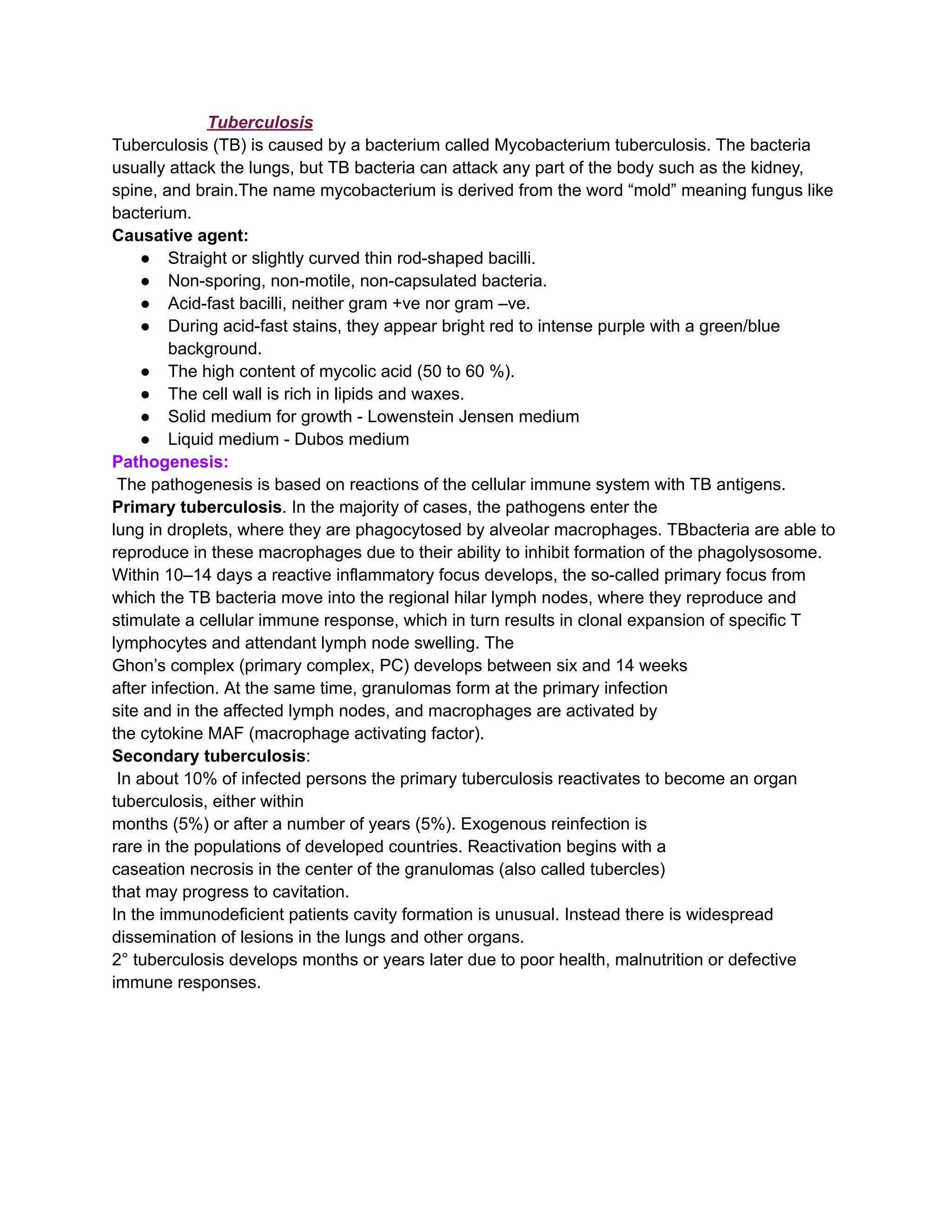
Primary tuberculosis. In the majority of cases, the pathogens enter the
lung in droplets, where they are phagocytosed by alveolar macrophages. TBbacteria are able to
reproduce in these macrophages due to their ability to inhibit formation of the phagolysosome.
Within 10–14 days a reactive inflammatory focus develops, the so-called primary focus from
which the TB bacteria move into the regional hilar lymph nodes, where they reproduce and
stimulate a cellular immune response, which in turn results in clonal expansion of specific T
lymphocytes and attendant lymph node swelling. The
Ghon’s complex (primary complex, PC) develops between six and 14 weeks
after infection. At the same time, granulomas form at the primary infection
site and in the affected lymph nodes, and macrophages are activated by
the cytokine MAF (macrophage activating factor).
Secondary tuberculosis:
In about 10% of infected persons the primary tuberculosis reactivates to become an organ
tuberculosis, either within
months (5%) or after a number of years (5%). Exogenous reinfection is
rare in the populations of developed countries. Reactivation begins with a
caseation necrosis in the center of the granulomas (also called tubercles)
that may progress to cavitation.
In the immunodeficient patients cavity formation is unusual. Instead there is widespread
dissemination of lesions in the lungs and other organs.
2° tuberculosis develops months or years later due to poor health, malnutrition or defective
immune responses.
2.
Symptoms:
The symptoms includedry cough (main), as a disease progresses there is sputum production,
mixed with blood (known as hemoptysis), fever, sweating, malaise, fatigue, & weight loss comes
along with the further disease progression
The disease can also involve other organs such as bone, kidneys, brain, meninges & bowel.
Laboratory diagnosis:
Specimens:
Samples depends on the site of infection
PTB:- sputum,
Tubercular meningitis:- CSF
Genitourinary TB:- urine.
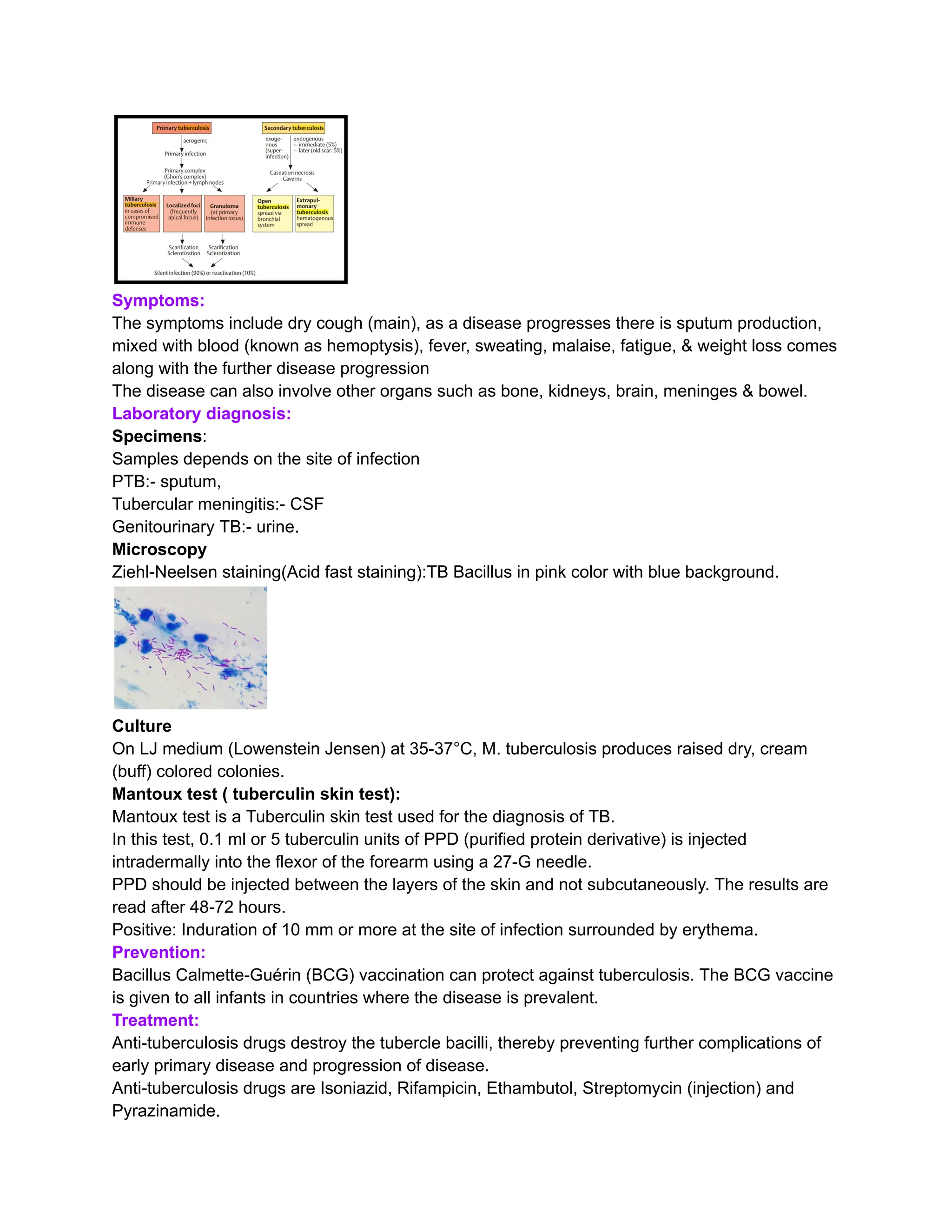
Microscopy
Ziehl-Neelsen staining(Acid fast staining):TB Bacillus in pink color with blue background.
Culture
On LJ medium (Lowenstein Jensen) at 35-37°C, M. tuberculosis produces raised dry, cream
(buff) colored colonies.
Mantoux test ( tuberculin skin test):
Mantoux test is a Tuberculin skin test used for the diagnosis of TB.
In this test, 0.1 ml or 5 tuberculin units of PPD (purified protein derivative) is injected
intradermally into the flexor of the forearm using a 27-G needle.
PPD should be injected between the layers of the skin and not subcutaneously. The results are
read after 48-72 hours.
Positive: Induration of 10 mm or more at the site of infection surrounded by erythema.
Prevention:
Bacillus Calmette-Guérin (BCG) vaccination can protect against tuberculosis. The BCG vaccine
is given to all infants in countries where the disease is prevalent.
Treatment:
Anti-tuberculosis drugs destroy the tubercle bacilli, thereby preventing further complications of
early primary disease and progression of disease.
Anti-tuberculosis drugs are Isoniazid, Rifampicin, Ethambutol, Streptomycin (injection) and
Pyrazinamide.
3.
Typhoid
Typhoid fever, alsoknown as enteric fever, is a potentially fatal multisystemic illness caused
primarily by Salmonella enterica, subspecies enterica serovar typhi and, to a lesser extent,
related serovars paratyphi A, B, and C.
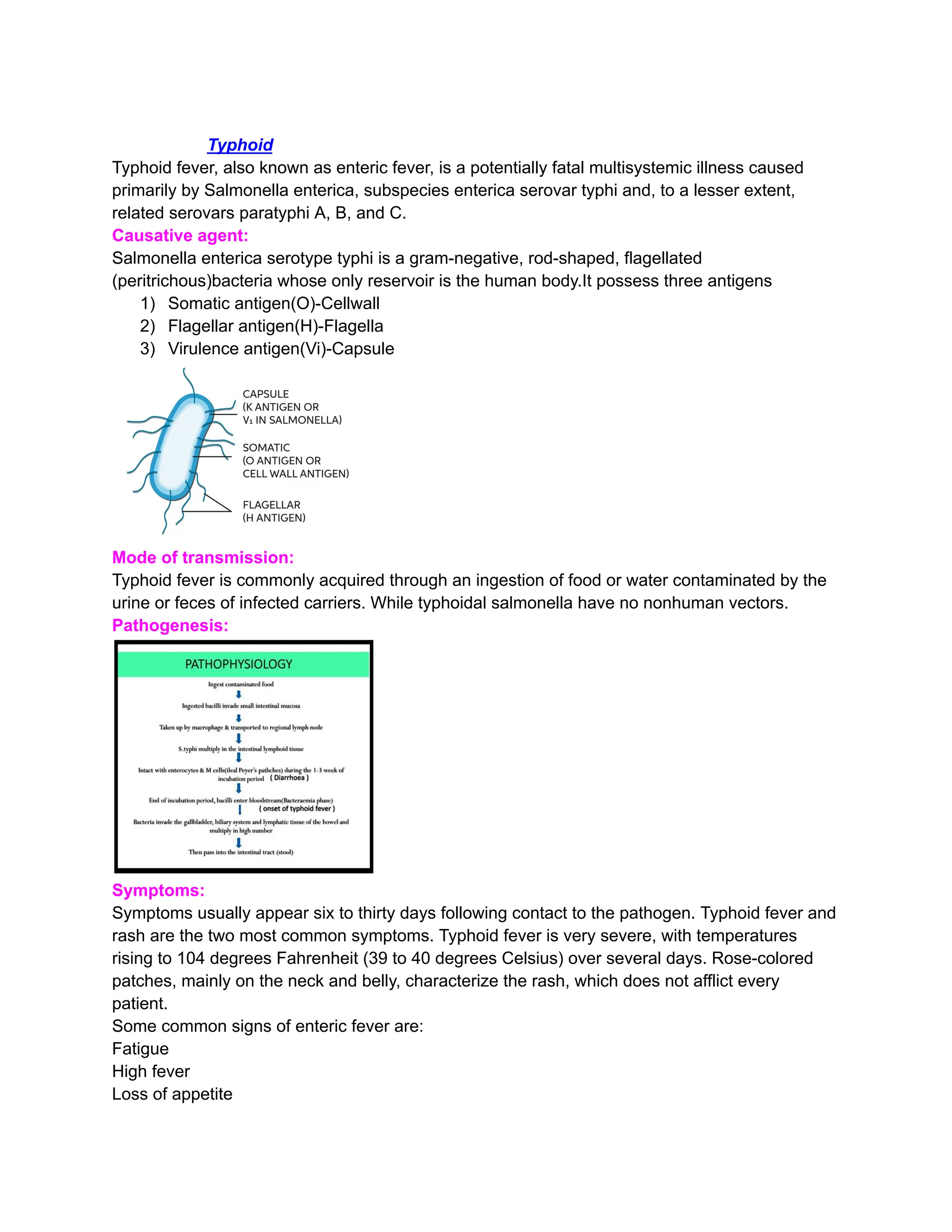
Causative agent:
Salmonella enterica serotype typhi is a gram-negative, rod-shaped, flagellated
(peritrichous)bacteria whose only reservoir is the human body.It possess three antigens
1) Somatic antigen(O)-Cellwall
2) Flagellar antigen(H)-Flagella
3) Virulence antigen(Vi)-Capsule
Mode of transmission:
Typhoid fever is commonly acquired through an ingestion of food or water contaminated by the
urine or feces of infected carriers. While typhoidal salmonella have no nonhuman vectors.
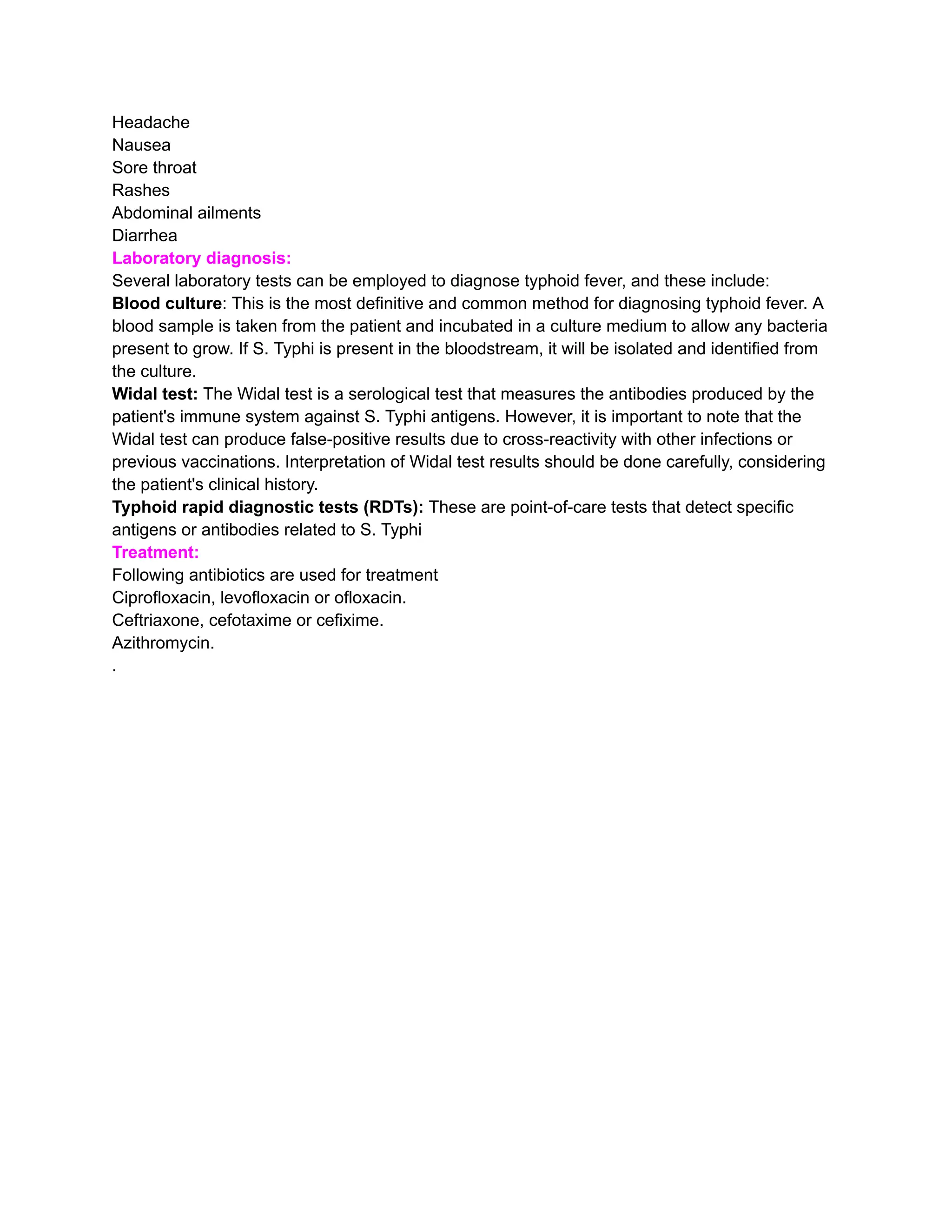
Pathogenesis:
Symptoms:
Symptoms usually appear six to thirty days following contact to the pathogen. Typhoid fever and
rash are the two most common symptoms. Typhoid fever is very severe, with temperatures
rising to 104 degrees Fahrenheit (39 to 40 degrees Celsius) over several days. Rose-colored
patches, mainly on the neck and belly, characterize the rash, which does not afflict every
patient.
Some common signs of enteric fever are:
Fatigue
High fever
Loss of appetite
4.
Headache
Nausea
Sore throat
Rashes
Abdominal ailments
Diarrhea
Laboratorydiagnosis:
Several laboratory tests can be employed to diagnose typhoid fever, and these include:
Blood culture: This is the most definitive and common method for diagnosing typhoid fever. A
blood sample is taken from the patient and incubated in a culture medium to allow any bacteria
present to grow. If S. Typhi is present in the bloodstream, it will be isolated and identified from
the culture.
Widal test: The Widal test is a serological test that measures the antibodies produced by the
patient's immune system against S. Typhi antigens. However, it is important to note that the
Widal test can produce false-positive results due to cross-reactivity with other infections or
previous vaccinations. Interpretation of Widal test results should be done carefully, considering
the patient's clinical history.
Typhoid rapid diagnostic tests (RDTs): These are point-of-care tests that detect specific
antigens or antibodies related to S. Typhi
Treatment:
Following antibiotics are used for treatment
Ciprofloxacin, levofloxacin or ofloxacin.
Ceftriaxone, cefotaxime or cefixime.
Azithromycin.
.