Introduction
• Hypersensivity reactionsare defined as any of the
following:
• Hypersensitivity reactions are excessive immune
responses leading to damage in the host.
• These are inappropriate immune responses
resulting in pathological changes in the host.
• Inappropriate responses to innocuous foreign
substances are called allergy or hypersensitivity
reactions.
3.
Classification
• Classification
• Historicallythese are divided on a time basis:
• Immediate reaction: Reaction develops in less than 24 hours.
• Delayed reaction: When reaction develops within 24-48 hours.
• Coomb’s and Gell classification: This was given in 1963.
• Ab-dependant reactions (B-L dependant)
• Type I = Anaphylactic and immediate reaction.
• Type II = Cytotoxic reaction.
• Type III = Immune-complex disease.
• Ab-independent reaction (T- L dependant)
• Type IV = Delayed or cell-mediated immunity.
4.
Type 1 Hypersensitivity
•This is also called immediate hypersensitivity when
an IgE response is directed against the antigens like
pollens and leads to the release of pharmacological
mediators, such as histamine IgE-sensitized mast
cells, and produces an acute inflammatory reaction
with S/S like asthma or rhinitis.
• This type 1 reaction can range from the life-
threatening anaphylactic reaction to milder forms
associated with food allergies.
• Atopic allergy, including hay fever, asthma, and
food allergy
5.
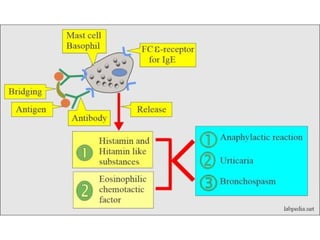
• This reactiontakes place in two stages:
• First Stage: This is the stage where there is
sensitization of the host and formation of IgE Ab,
which, once formed, attaches to the receptors on
mast cells or basophil.
• Second Stage: This is the stage of reaction or
shocking dose in this stage where patients will
have histamine effects and called histamine
poisoning.
7.
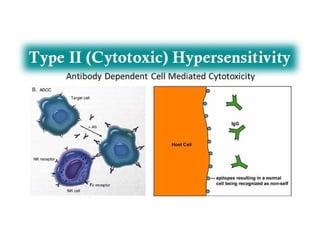
Type 11 Hypersensitivity
•Type II hypersensitivity reaction refers to an
antibody-mediated immune reaction in which
antibodies (IgG or IgM) are directed against
cellular or extracellular matrix antigens with the
resultant cellular destruction, functional loss, or
damage to tissues. Damage can be accomplished
via three different mechanisms:
• Antibody binding to cell surface receptors and
altering its activity
• Activation of the complement pathway.
• Antibody dependant cellular cytotoxicity.
8.
• Examples ofType II Hypersensitivity
• Rhesus incompatibility (Rh hemolytic disease)
• During subsequent pregnancies, when Rh –ve mother
conceive Rh +ve fetus, small numbers of fetal
erythrocytes that pass across the placenta stimulate a
memory response which results in IgG antibodies
destroying the fetal erythrocytes (hemolytic disease of
the newborn).
• Transfusion Reactions
• Natural antibodies to major blood group antigens (A,
B) bind to transfused erythrocytes carrying the target
antigens resulting in massive hemolysis.
9.
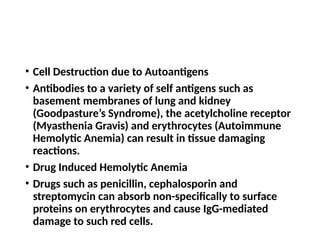
• Cell Destructiondue to Autoantigens
• Antibodies to a variety of self antigens such as
basement membranes of lung and kidney
(Goodpasture’s Syndrome), the acetylcholine receptor
(Myasthenia Gravis) and erythrocytes (Autoimmune
Hemolytic Anemia) can result in tissue damaging
reactions.
• Drug Induced Hemolytic Anemia
• Drugs such as penicillin, cephalosporin and
streptomycin can absorb non-specifically to surface
proteins on erythrocytes and cause IgG-mediated
damage to such red cells.
11.
Type 111 Hypersensitivity
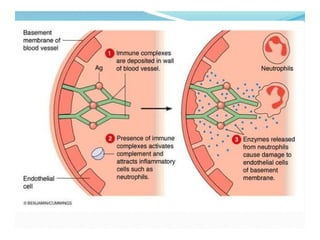
•In type III hypersensitivity reaction, an abnormal
immune response is mediated by the formation of
antigen-antibody aggregates called "immune
complexes." They can precipitate in various tissues
such as skin, joints, vessels, or glomeruli, and
trigger the classical complement pathway.
Complement activation leads to the recruitment
of inflammatory cells (monocytes and neutrophils)
that release lysosomal enzymes and free radicals
at the site of immune complexes, causing tissue
damage.
12.
Factors influencing Type111
Hypersensitivity
• 1. Persistent infection:
• In persistent infection such as Malaria, large number of
immune complexes are formed and deposited in tissues.
• 2. Complement deficiency:
• Complement removes immune complexes from blood, but
when complement system is deficient, large amount of
immune complexes circulates in blood and deposits in tissues.
• 3. Autoimmunity:
• In autoimmune disease, large amount of immune complexes
are formed and deposited in tissues.
• 4. Genetic defects:
• In certain genetic defects, small and soluble immune complexes
are formed that can not be phagocytosed.
13.
Types
• 1. LocalizedType III hypersensitivity reaction:
• Acute Arthus reaction is an example of localized
Type III hypersensitivity reaction.
• When antigen is injected or enters intradermally
or subcutaneously, they bind with antibody to
form localized immune complexes which mediate
acute Arthus reaction within 4 to 8 hours.
• As the reaction develops, localized tissue damage
and vascular damage results in accumulation of
fluids (edema) and RBCs (erythema) at the site of
antigen entry.
14.
• 2. GeneralizedType III hypersensitivity reaction:
• Serum sickness is an example of generalized Type III
hypersensitivity reaction.
• When large amount of antigen enter blood stream and
bind to antibody, circulating immune complexes forms.
If antigens are in significantly excess compared to
antibody, the immune complexes formed are smaller
and soluble which are not phagocytosed by phagocytic
cells leading to Type III hypersensitivity reaction.
• The manifestation of serum sickness depends on the
quantity of immune complex as well as overall site of
deposition. The site may vary but accumulation of
complexes occurs at site of blood filtration.
16.
Type 1V Hypersensitivity
•Type IV hypersensitivity reaction also knowTypn
as cell mediated hypersensitivity or delayed type
of hypersensitivity is the T lymphocytes mediated
destruction of cells along with dendritic cells,
macrophages and cytokines playing major roles.
• The reaction is mediated by specific subsets of
CD4+ helper T cells (Th-1 and Th-17 cells) or by
CD8+ cytotoxic T cells.
• Type IV hypersensitivity occurs 24 hours after
contact with an antigen, usually starting at 2 or 3
days and often last for many days.
17.
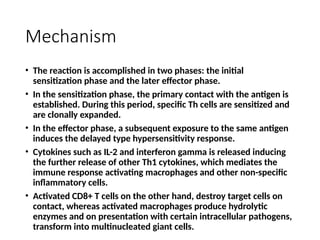
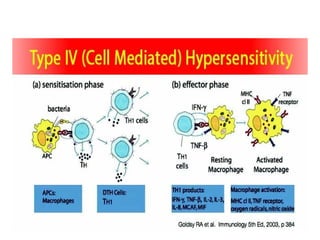
Mechanism
• The reactionis accomplished in two phases: the initial
sensitization phase and the later effector phase.
• In the sensitization phase, the primary contact with the antigen is
established. During this period, specific Th cells are sensitized and
are clonally expanded.
• In the effector phase, a subsequent exposure to the same antigen
induces the delayed type hypersensitivity response.
• Cytokines such as IL-2 and interferon gamma is released inducing
the further release of other Th1 cytokines, which mediates the
immune response activating macrophages and other non-specific
inflammatory cells.
• Activated CD8+ T cells on the other hand, destroy target cells on
contact, whereas activated macrophages produce hydrolytic
enzymes and on presentation with certain intracellular pathogens,
transform into multinucleated giant cells.
18.
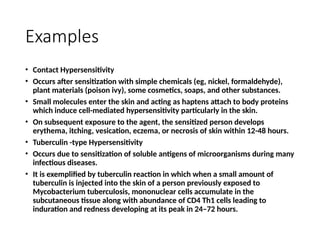
Examples
• Contact Hypersensitivity
•Occurs after sensitization with simple chemicals (eg, nickel, formaldehyde),
plant materials (poison ivy), some cosmetics, soaps, and other substances.
• Small molecules enter the skin and acting as haptens attach to body proteins
which induce cell-mediated hypersensitivity particularly in the skin.
• On subsequent exposure to the agent, the sensitized person develops
erythema, itching, vesication, eczema, or necrosis of skin within 12-48 hours.
• Tuberculin -type Hypersensitivity
• Occurs due to sensitization of soluble antigens of microorganisms during many
infectious diseases.
• It is exemplified by tuberculin reaction in which when a small amount of
tuberculin is injected into the skin of a person previously exposed to
Mycobacterium tuberculosis, mononuclear cells accumulate in the
subcutaneous tissue along with abundance of CD4 Th1 cells leading to
induration and redness developing at its peak in 24–72 hours.