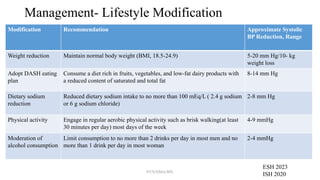
Hypertension affects 1.28 billion adults globally, with prevalence varying by age and gender. The document outlines hypertension's definition, classification, management strategies, and critical recommendations for diagnosing and addressing hypertensive emergencies. Emphasis is placed on lifestyle modifications, treatment combinations, and the importance of early detection and control of blood pressure.











































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



