
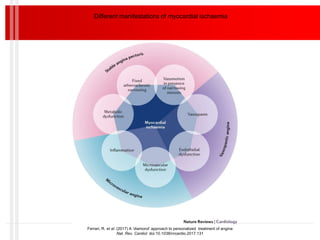
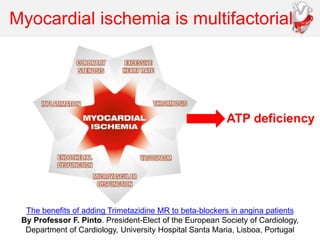
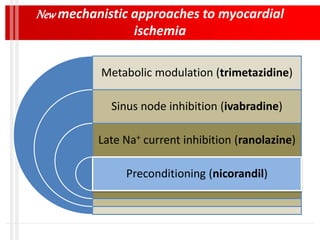
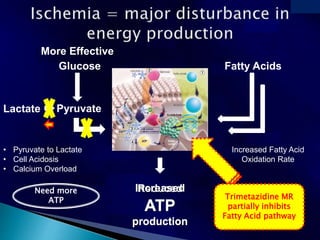
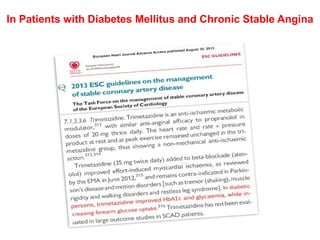
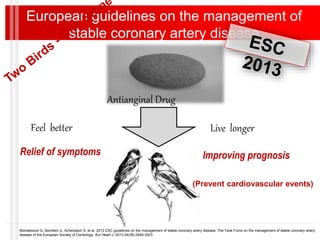
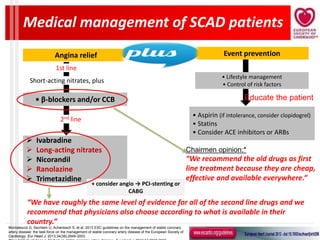
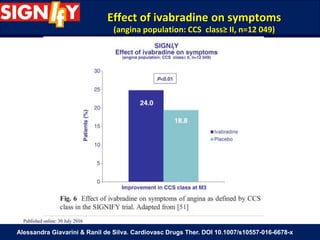
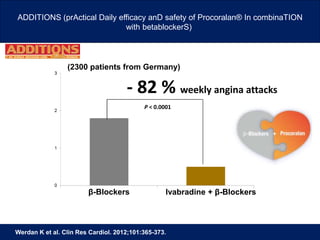
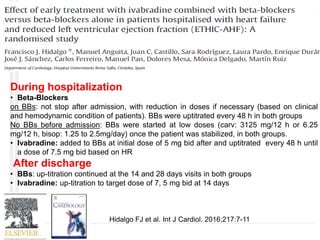
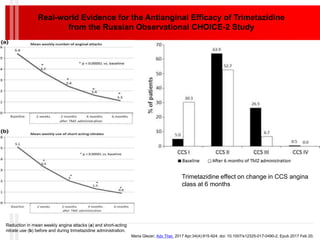
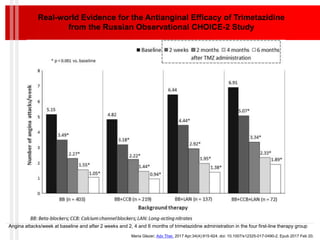
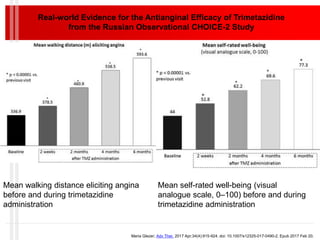

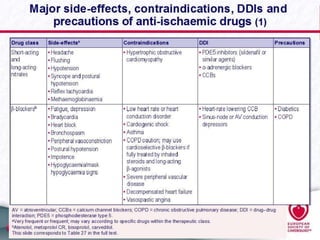
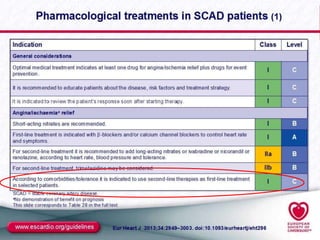
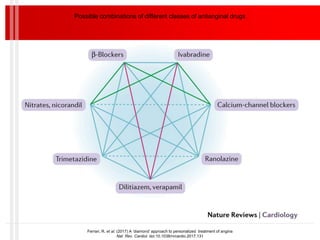
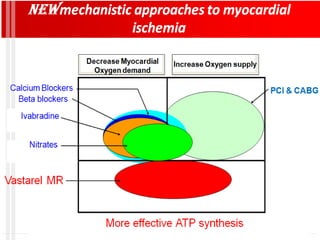
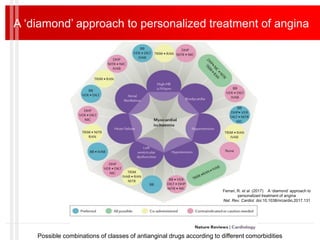

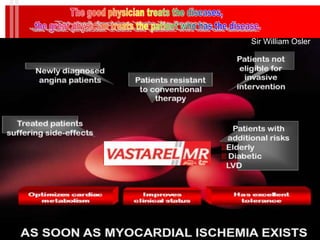


The document discusses stable ischemic heart disease and new approaches for its treatment. It summarizes several studies comparing different drug combinations for treating angina, finding that combining multiple hemodynamic drugs provides no additional benefit over monotherapy. Newer drugs like ivabradine, ranolazine, and trimetazidine are discussed as alternatives for treating angina by non-hemodynamic mechanisms like metabolic modulation. Trimetazidine in particular is highlighted for its efficacy in reducing angina symptoms and improving quality of life in real-world clinical studies. The document advocates for more personalized treatment approaches combining different drug classes tailored to individual patient characteristics and comorbidities.




































![7. Ischaemic Heart Disease and Acute Coronary Syndromes [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/7-251128082316-c3f9588b-thumbnail.jpg?width=640&height=640&fit=bounds)


















































