Major histocompatibility complex
Group of genes coding for a set of host surface molecules that bind to a
peptide fragments derived from pathogens and foreign antigens, and
display them on host cell surface for recognition by the appropriate T
cells.
Also called human leukocyte antigens (HLA).
Serves as a unique identification marker for every individual.
Following transplantation of a graft the recipient mount an immune
response against the graft’s MHC molecules and vice versa.
Also called histocompatibility antigens.
3.
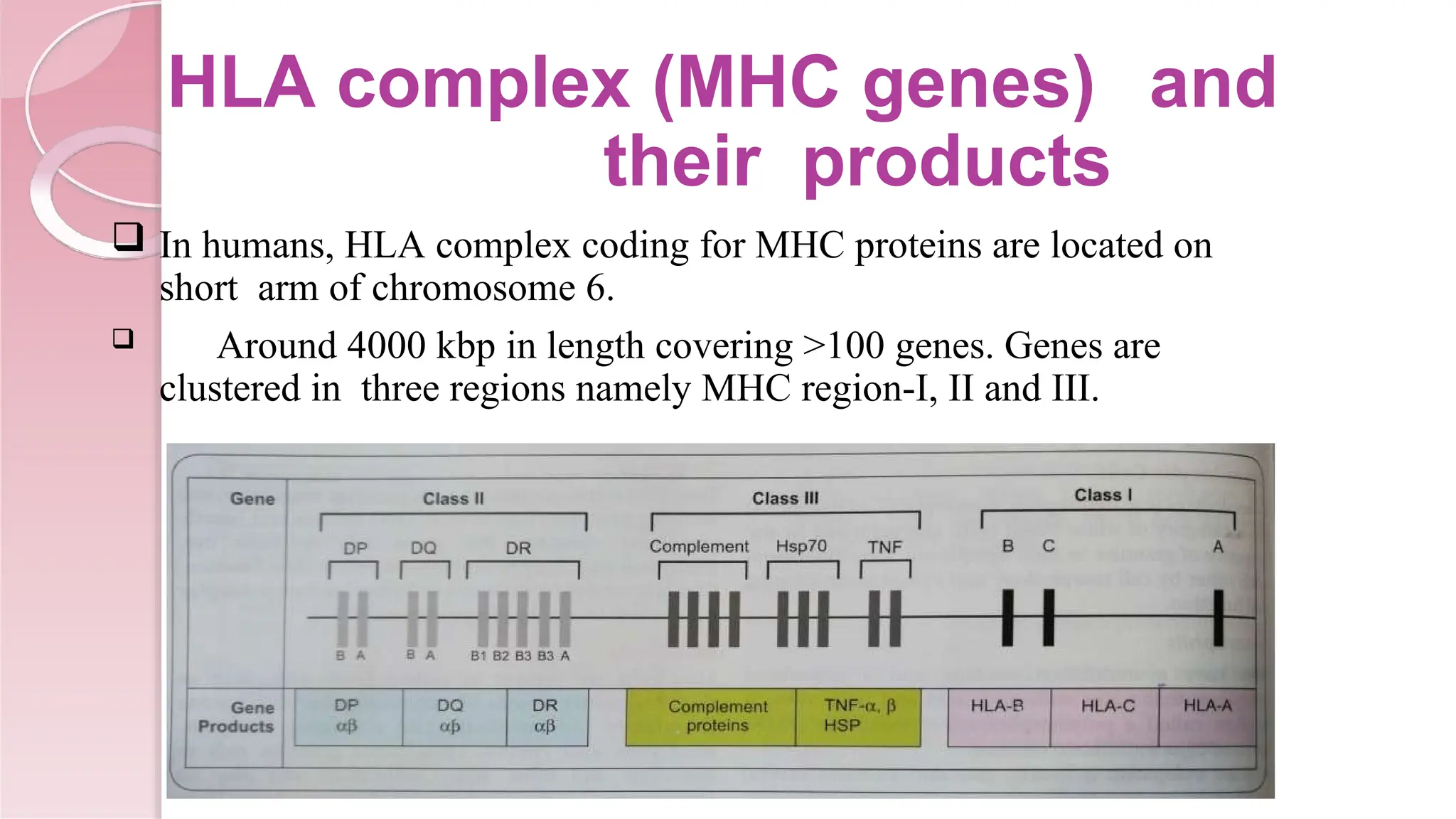
HLA complex (MHCgenes) and
their products
In humans, HLA complex coding for MHC proteins are located on
short arm of chromosome 6.
Around 4000 kbp in length covering >100 genes. Genes are
clustered in three regions namely MHC region-I, II and III.
4.
MHC region I
About 2000 kbp in length. Comprises of three class I genes called
HLA-A, HLA-B and HLA-C genes encoding HLA-A, HLA-B and
HLA-C proteins respectively.
Each protein is capable of forming the α-chain of MHC class I
molecules.
MHC class I molecules are present on the surface of all nucleated
cells (except sperm cells) and platelets.
Present the peptide antigen to CD8+ T cells.
5.
MHC region II
About 1000 kbp length. Comprises of three genes namely DP, DQ and DR genes
encoding DP, DQ and DR proteins respectively.
Each protein is capable of forming α and β-chain of MHC class II molecules.
In addition MHC region also contain non classical genes such as DM, DO,
LMP and TAP that help in antigen processing and presentation.
MHC-II proteins are located on the surface of APC.
Present the peptide to CD4+ T cells.
6.
MHC region III
About 1000 kbp in length. Not involved in Ag presentation.
Comprises of genes that code for complement factors, heat shock
proteins (HSP), tumor necrosis factor (TNF α and β), steroid 21
hydroxylases etc.
7.
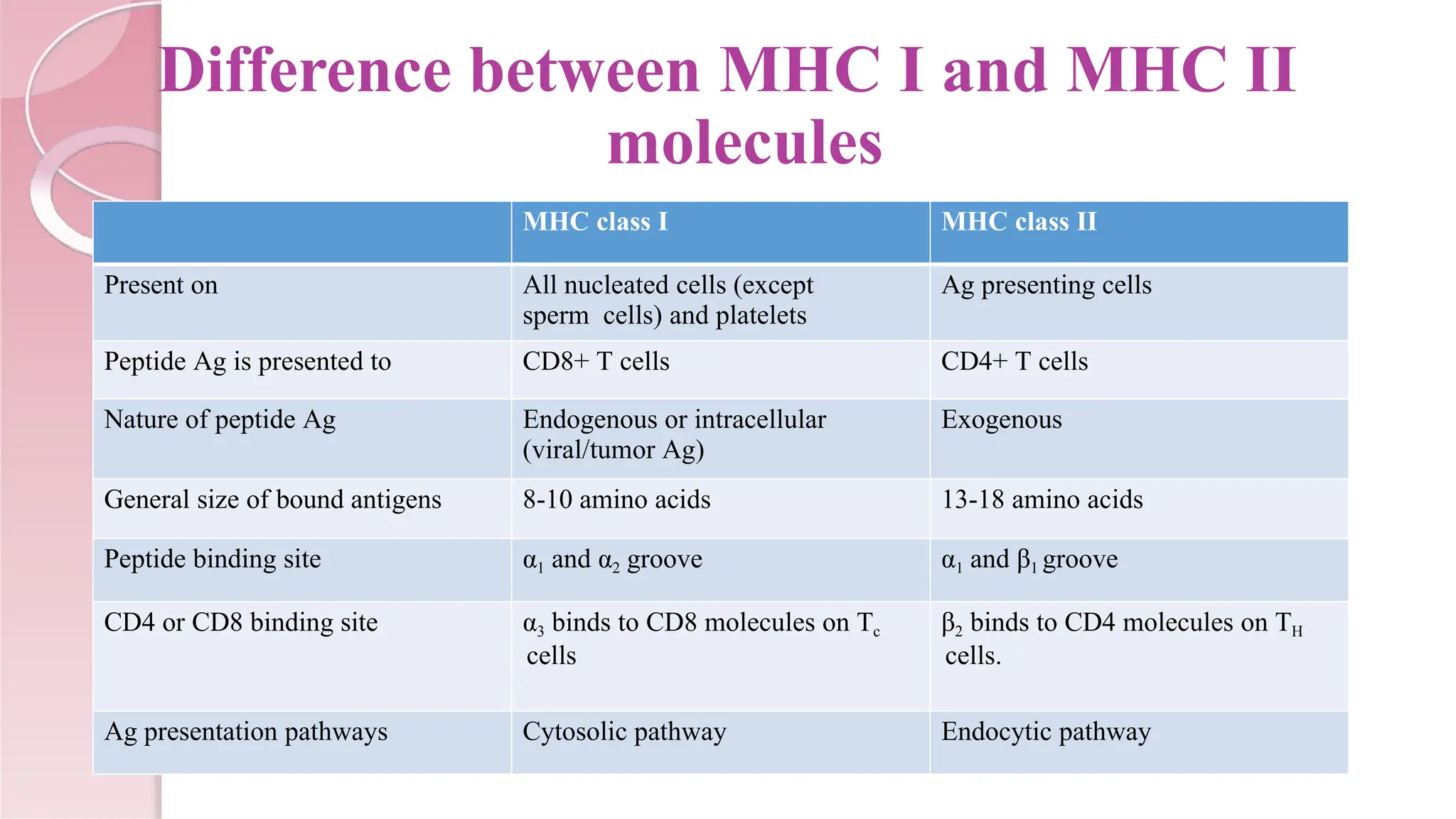
Difference between MHCI and MHC II
molecules
MHC class I MHC class II
Present on All nucleated cells (except
sperm cells) and platelets
Ag presenting cells
Peptide Ag is presented to CD8+ T cells CD4+ T cells
Nature of peptide Ag Endogenous or intracellular
(viral/tumor Ag)
Exogenous
General size of bound antigens 8-10 amino acids 13-18 amino acids
Peptide binding site α1 and α2 groove α1 and β1 groove
CD4 or CD8 binding site α3 binds to CD8 molecules on Tc
cells
β2 binds to CD4 molecules on TH
cells.
Ag presentation pathways Cytosolic pathway Endocytic pathway
8.
HLA
TYPING
In thistest, donor’s antigens expressed on the surface of leukocytes or
their genes are matched with that of the recipient.
The closer the HLA antigens on the transplanted organ match the
recipient, the more likely that the recipient’s body will not reject the
transplant.
Value of HLA matching between donor and recipient varies in different
solid organ transplantation. In kidney transplants, there is substantial
benefit if all the polymorphic HLA alleles are matched.
9.
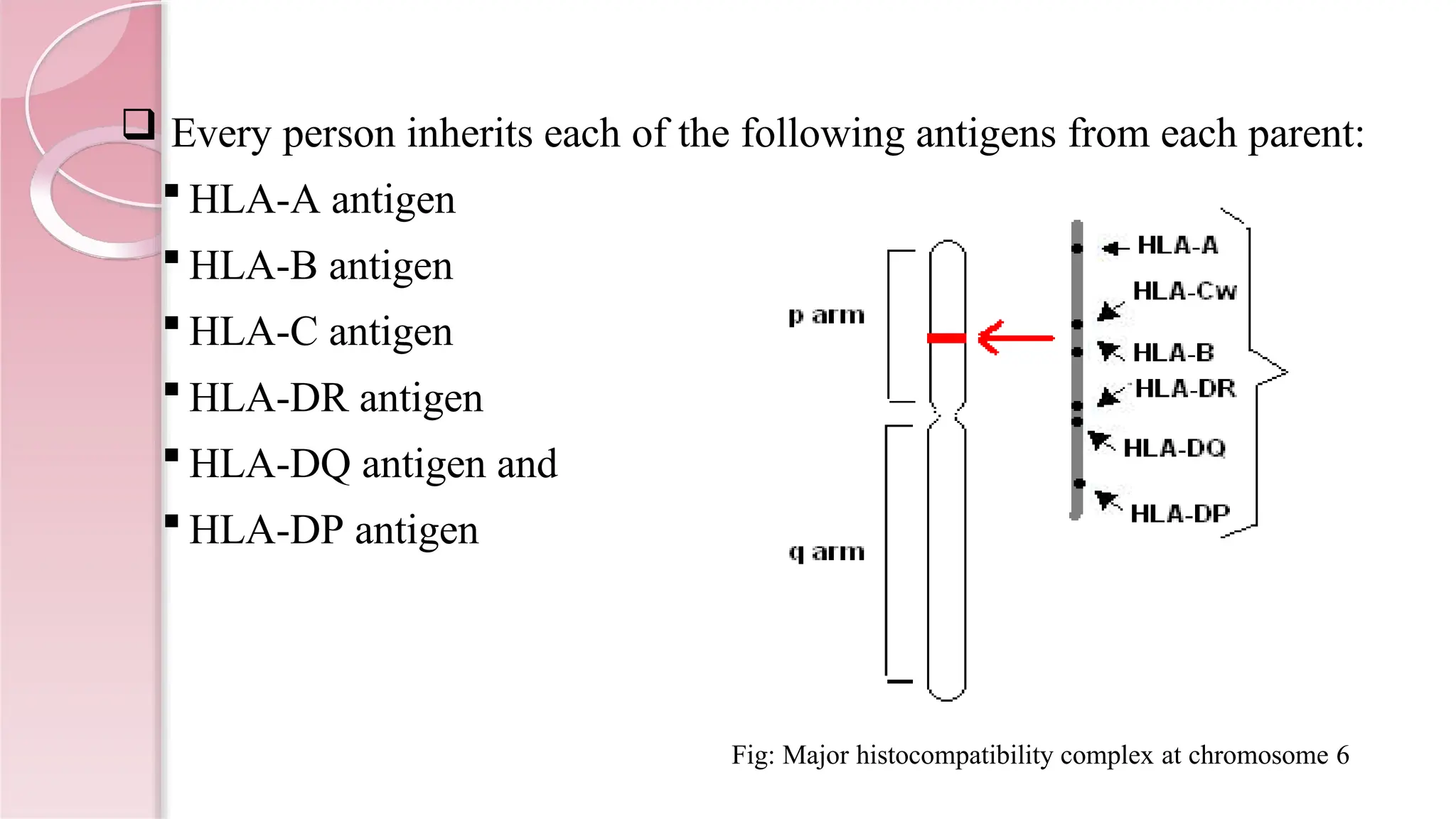
Every personinherits each of the following antigens from each parent:
HLA-A antigen
HLA-B antigen
HLA-C antigen
HLA-DR antigen
HLA-DQ antigen and
HLA-DP antigen
Fig: Major histocompatibility complex at chromosome 6
10.
When performingan HLA typing test for a kidney transplant,
the following HLA antigens are looked at:
HLA-A
HLA-B
HLA-DR
Six HLA antigens are looked at for each person.
11.
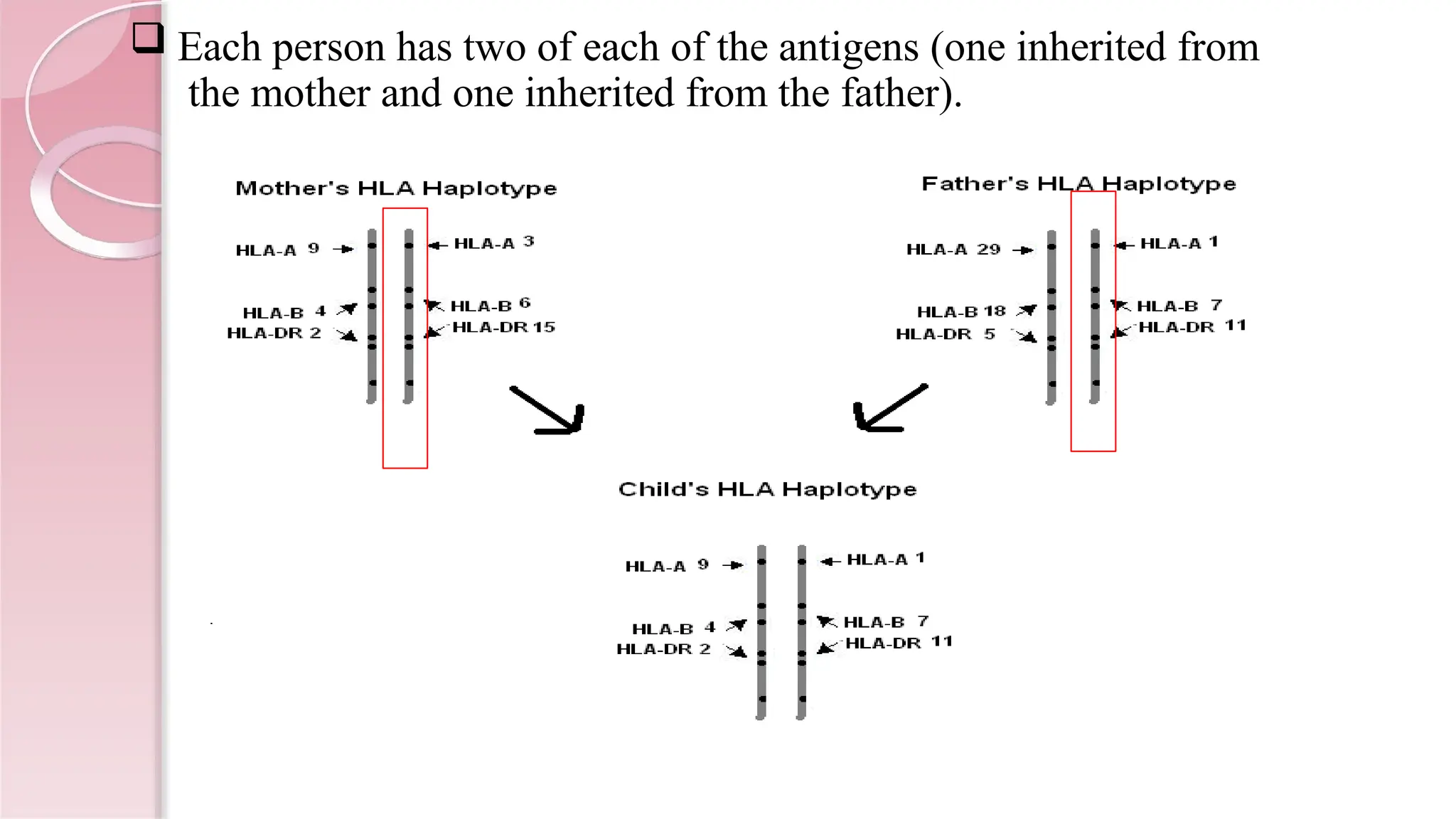
Each personhas two of each of the antigens (one inherited from
the mother and one inherited from the father).
12.
By analyzingwhich six of these HLA-antigens both the donor and
recipient have, scientists are able to determine the closeness of
tissue matching.
A six-antigen match is the best compatibility between a donor and
recipient.
This match occurs 25% of the time between siblings who have the
same mother and father.
13.
METHODS OF HLA
TYPING
A.Phenotypic method:
Serology: Microcytotoxicity
Tissue typing: Mixed lymphocyte reaction
B. Genotypic methods:
PCR detecting HLA genes
PCR-RFLP (restriction fragment length polymorphism)
Variable number tandem repeat (VNTR) typing
Short tandem repeat (STR) typing
DNA sequence based typing
Karyosome analysis
14.
Serology: Microlymphocytotoxic
test:
ViableWBC’s of the individual to be typed are
incubated with HLA (class I and II) specific antibodies.
If the specific Ag is present on the cell, the antibody is
bound.
Complement is added and incubated.
If the antibody is bound, it will activate the
complement which damages the cell membrane
making it permeable to vital stains.
15.
Pros Cons
Easily performed,does not require
expensive equipments
Require large volume of blood
3 hrs Require viable WBC’s
With good antisera results are reliable Difficult to find good antisera for rarer
antigens.
16.
1. Organ andtissue transplantation
In organ and tissue transplantation, HLA antigens of the donor
identified as invaders by the recipient causing rejection. Careful
selection of the matched donor and recipient critically affect
the outcome of transplantation.
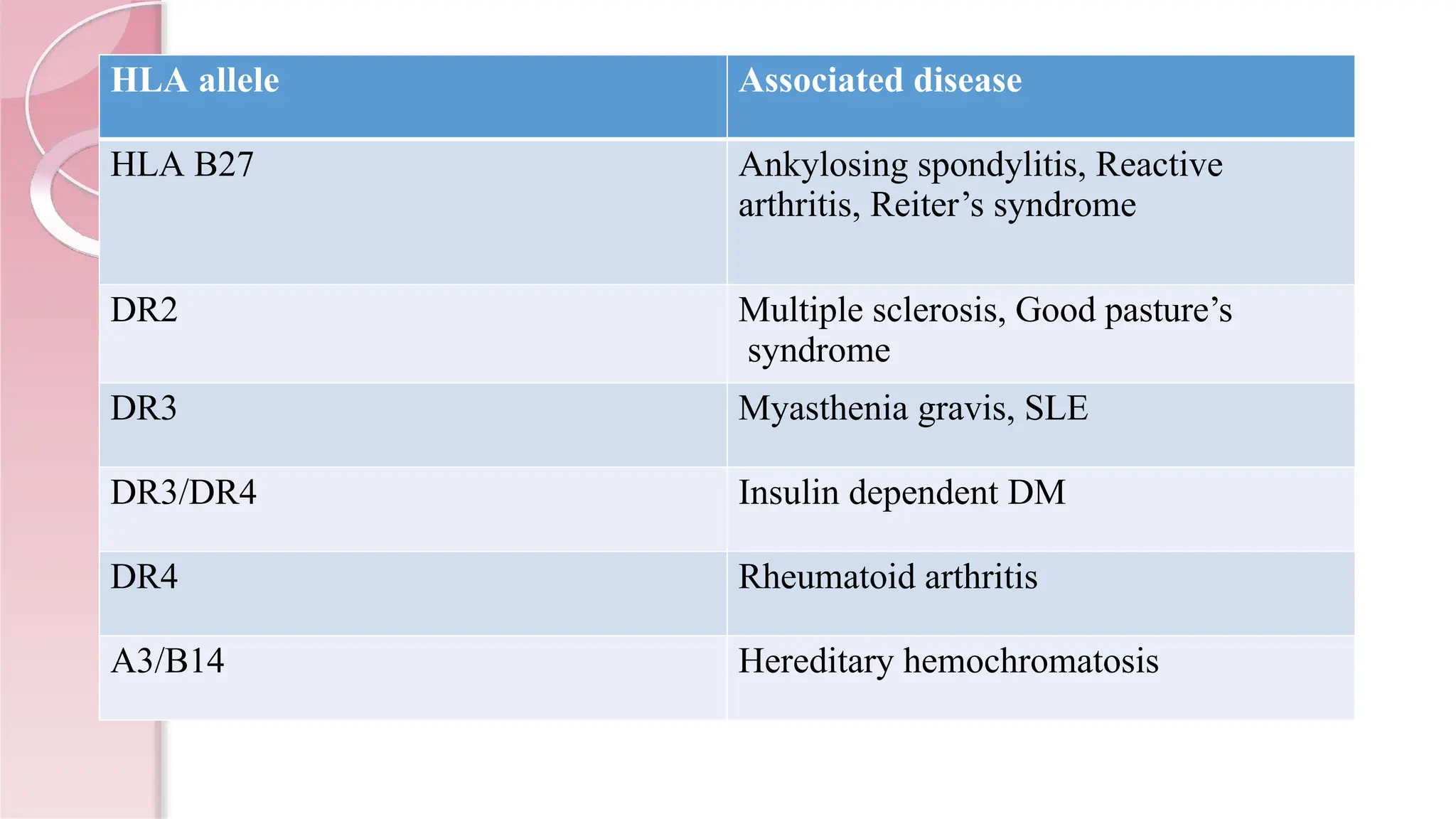
2. Diagnosing some disease :
In autoimmunity: Many HLA combination are potentially indicative
of autoimmune disorders, e.g.
Application of HLA
typing
Susceptibility toviral infections: There is a link between certain
HLA antigens and susceptibility to some viral infections such
as AIDS (HIV virus), Hepatitis B (Hep B), Hepatitis C (Hep
C), Infectious mononucleosis (EVB), Rubella (Rubella virus)
etc.
3. Paternal testing
HLA typing can be used alongside other test for paternity
testing.
19.
4. Infertility (recurrentpregnancy loss):
Infertility due to recurrent pregnancy loss can be attributed to
immune factors (40%) one of which is presence of certain common
HLA antigens between the parents.
5. Phylogenetic studies:
Some HLA haplotypes have distinctive geographical
distribution and are found only in some population. These
haplotypes can be used to trace human migration.
Protocol
Lymphocyte fromdonor are isolated and separated in to T and B cells
Serum from recipients is mixed with t-lymphocyte in multi-well plate
Complement is added (from rabbit serum)
If donor specific antibody is present it will bind to donor cells, then
complement cascade will be activated and results in lysis of T-
lymphocytes
Stain the cells
Observe cells under microscope
Red color indicates dead cells
Greenish yellow indicates live cells
Results can be calculated on the basis of score (calculate % of dead
cells to live cells)
0-no dead cells
2,4, 6- level of lysis
Principle
• Antibody secretingB lymphocytes can be enumerated
by their ability to bind to antigens present on RBCs.
• In presence of complement the antibody bound RBCs
are lyased
• The plaques thus formed can be detected using
benzidine reagent
• The peroxidase activity of Hb (released by the lysed
cells) decomposes hydrogen peroxidase and the
liberated active oxygen oxidizes benzidine to give blue
color
25.
Requirements
B cells fromperson with Blood gr. O
Sterile petri dish
Sterile 1% agar
RBCs from a person with Blood gr A or B
Complement (serum from O blood group person)
Benzidine reagent (Benzidine +acetic acid+H2O2)
26.
Protocol
Separate lymphocytesby Ficoll hypaque using blood group O
Separate B-cells by Fenwall wool
Remove test tube of agar from 50 0C water and place them in
a beaker filled with warm water
Add 0.5 ml of the B-cell suspension to the agar and mix the
contents
Add 0.1 ml of RBCs from A or B blood group person to each
tube and mix again
Quickly pour the contents into a petri dish that already has a
bottom layer of agar. Swirl the petri dishes in a figure eight to
obtain an even top layer, allow that agar to harden and then
incubate the plates at 37 0C for one hour
27.
Add 2ml of complement to the petri dish, swirl the dish
to distribute solution evenly and re-incubate at 37 0C for
30 min
Remove plates store at RT for 30-60 min, rinse and
store overnight
Stain by 8 ml benzidine reagent
Pour off stain and rinse and count plaques (light areas
on dark blue background)
Calculate number of plaques/ml of blood
Results: Assay was performed theoretically
Rodents and rabbitsare often used to produce antibodies for
various research activities
Certain guidelines have to be followed:
1. The immunizing material must be virtually free of toxic
substances (e.g. urea, acetic acid). It should present no risk
of pathogenicity or toxicity to the host animals in the colony,
or personnel
2. Injections for routine antibody production should be
administered subcutaneously in 2-4 sites per animal
3. All guidelines must be given for when and how all test must
be done
4. For bleeding, 10 % of blood volume
5. It is possible to produce substantial amounts of polyclonal
antibodies
6. Harvesting ascites
30.
7. Dis-infection isnecessary with 70% ethanol or betadine
8. Three taps per mouse may be performed
9. Mice that fail to produce ascites within 25 days after
hybridoma injection should be euthanized
Results: Practical was performed theoretically