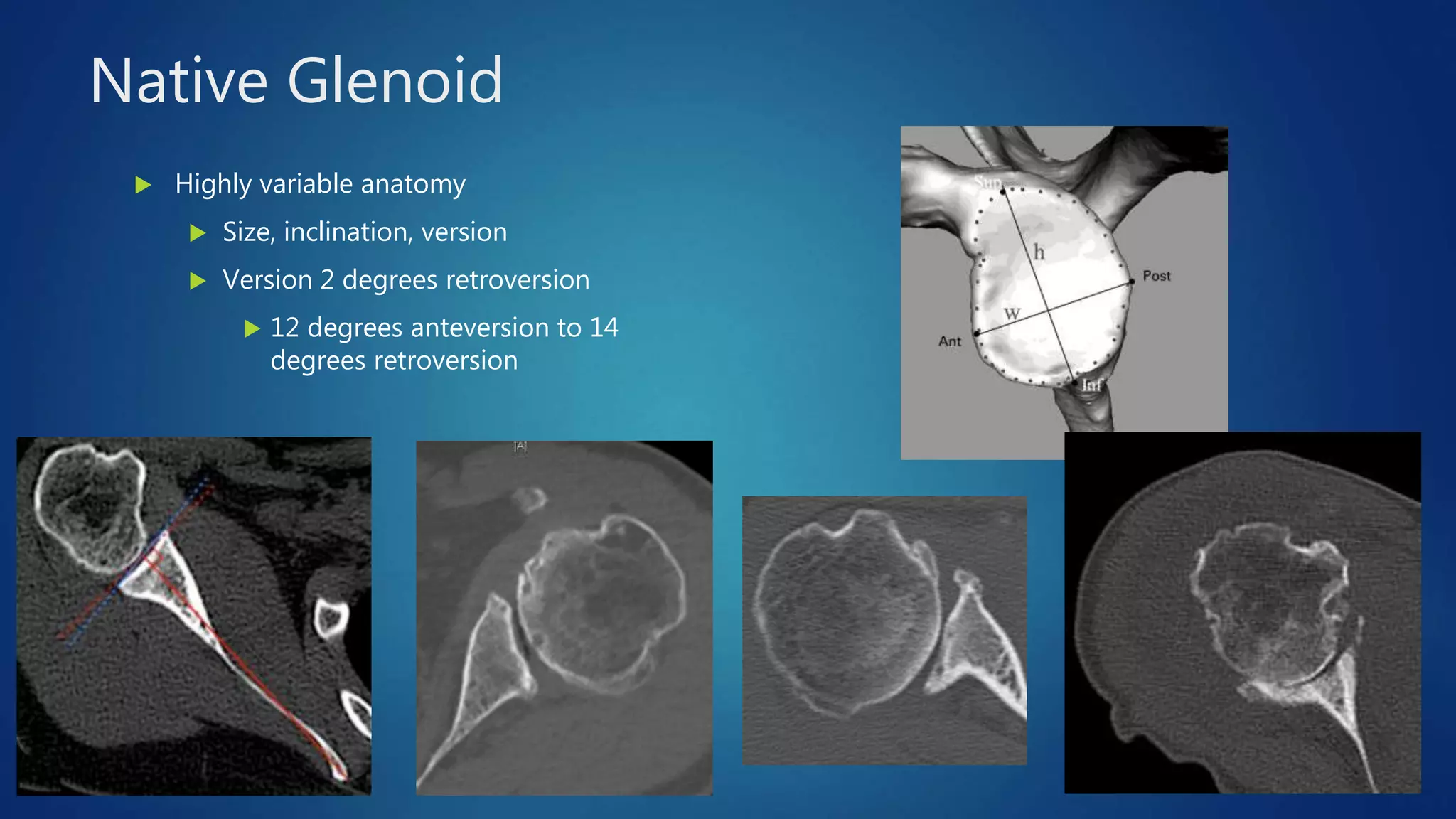
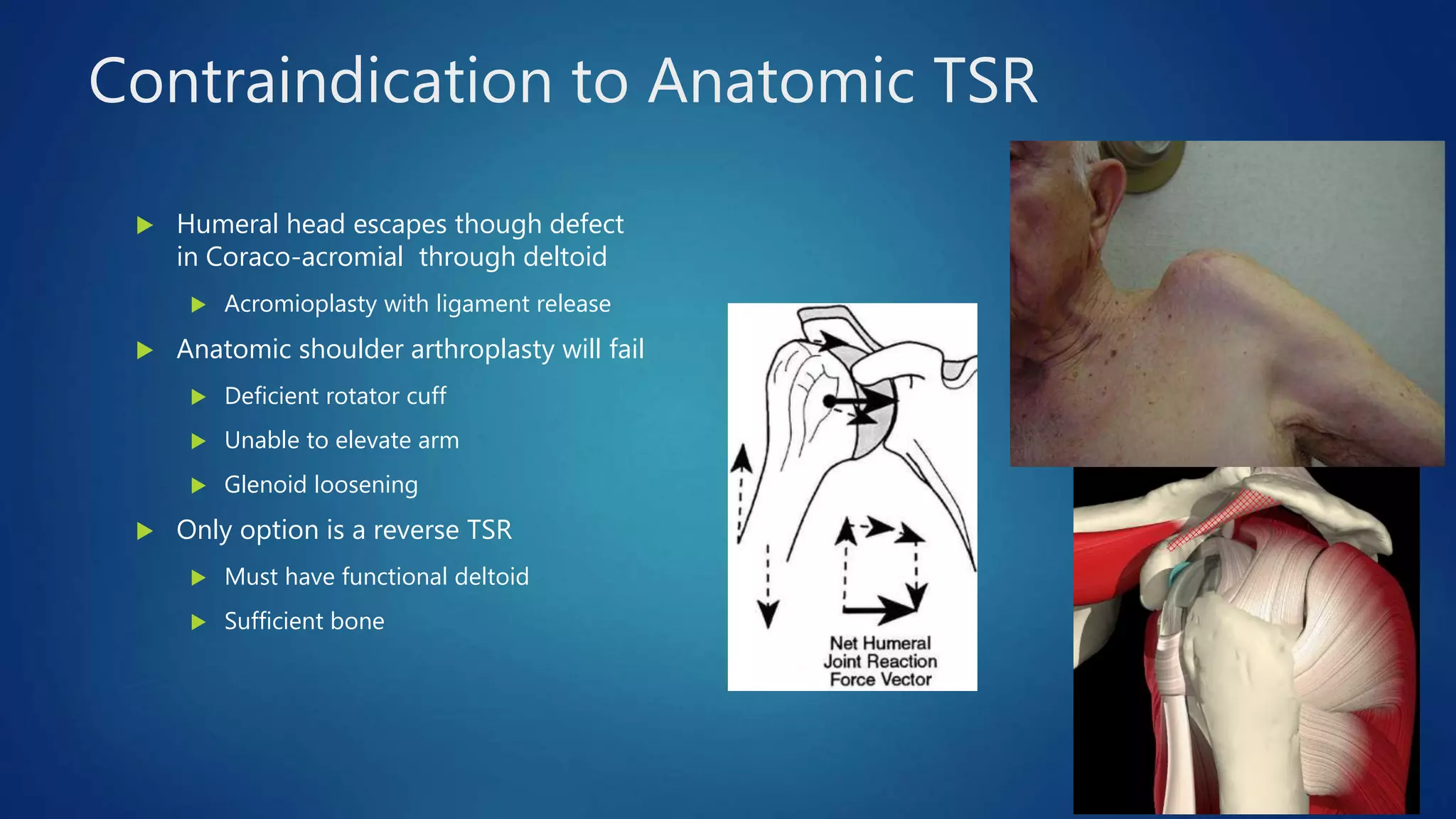
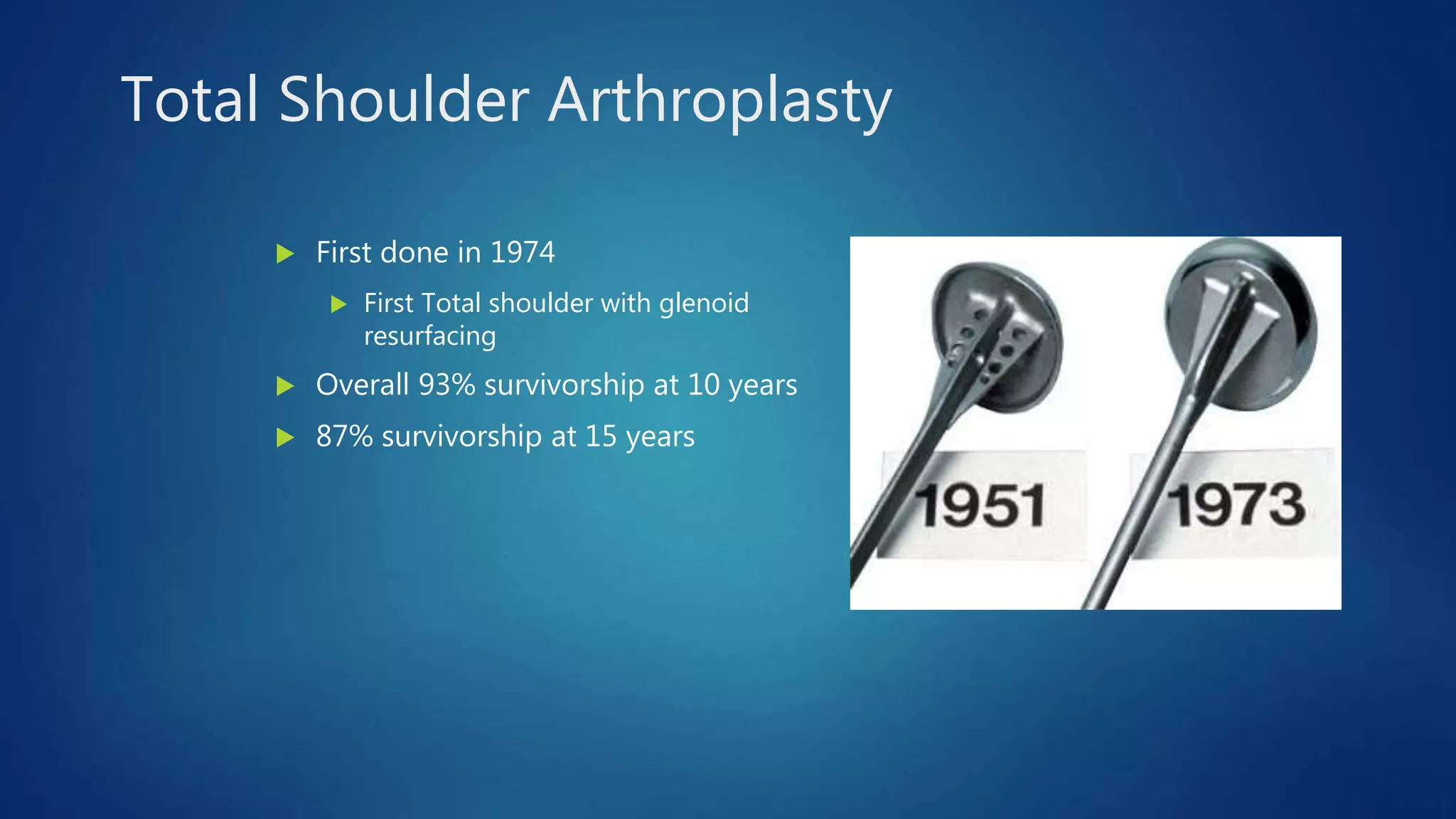
The document provides an overview of total shoulder arthroplasty, detailing the anatomy, function, and complications associated with shoulder replacements. It discusses indications for surgery, the differences between anatomic and reverse total shoulder arthroplasty, and highlights key statistics related to outcomes and recovery timelines. Additionally, it outlines factors influencing shoulder arthritis and rotator cuff tears as well as rehabilitation protocols post-surgery.




































































































![ROTATOR CUFF[4273].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/rotatorcuff4273-221222051719-751991ae-thumbnail.jpg?width=640&height=640&fit=bounds)




































