Download as PDF, PPTX














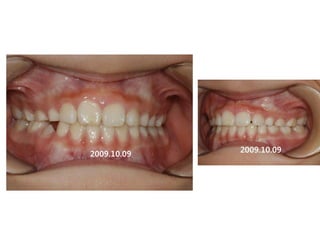
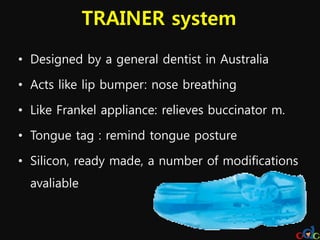






































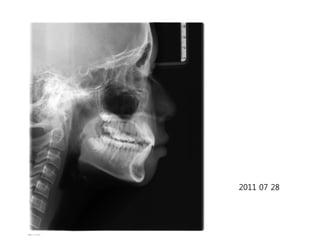
















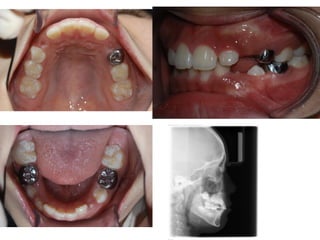

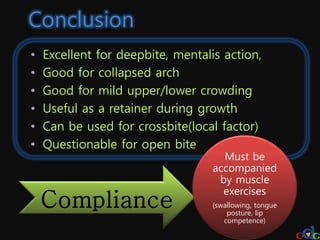

This document discusses the Trainer (T4K) appliance system, which is designed to address malocclusions caused by oral muscle imbalances. It acts like a lip bumper to encourage nose breathing and relieves buccinator muscle tension like a Frankel appliance. A tongue tag is also included to remind the wearer of proper tongue posture. Case studies are presented showing how T4K helped correct deep bites, crowding, crossbites and other issues by establishing normal swallowing and muscle function over periods ranging from 4 months to 2 years. Limitations include potential for gum irritation and difficulty enforcing compliance and fees. Proper muscle exercises are emphasized for best results.













































































