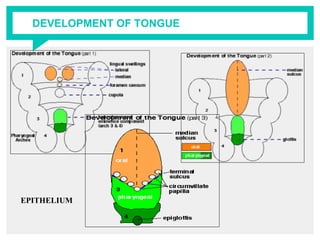
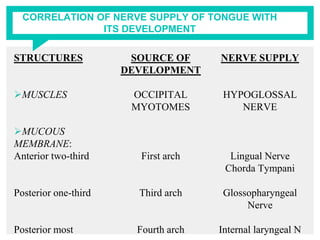
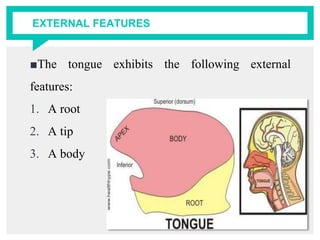
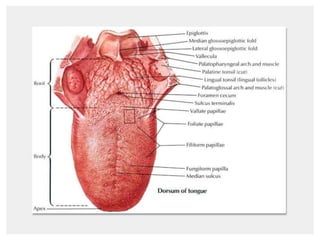
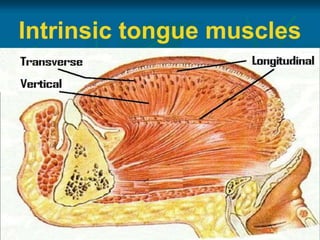
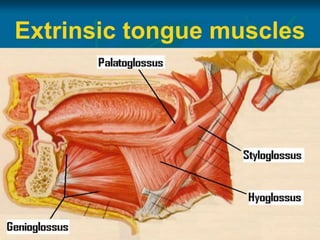
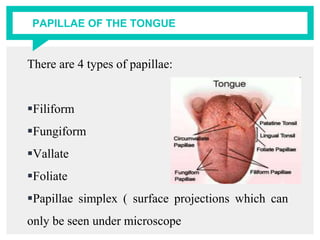
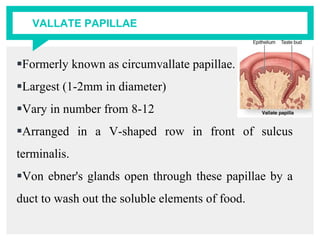
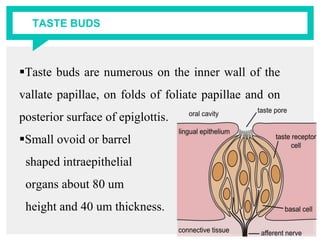
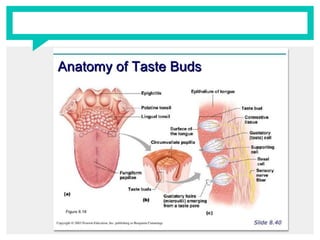
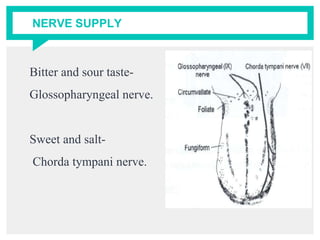
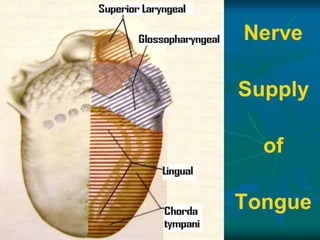
The document provides information about the anatomy and structures of the tongue. It begins with an introduction and then discusses the functions, development, external features, muscles, mucous membrane, glands, nerve supply, examination, and diseases of the tongue. The document contains detailed descriptions of the intrinsic and extrinsic tongue muscles, papillae, taste buds, arterial supply, lymphatic and venous drainage, and how to properly examine the tongue.



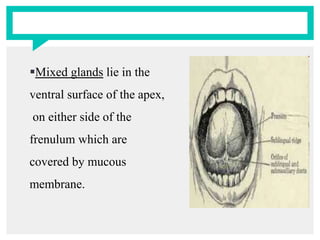


























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)














