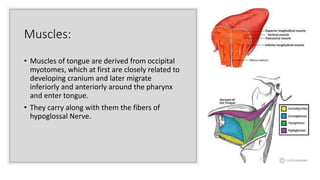
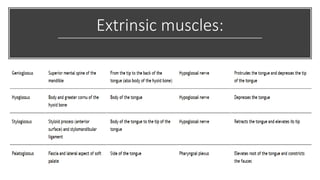
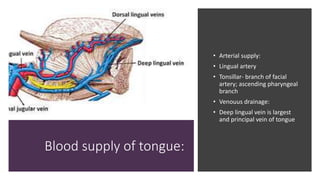
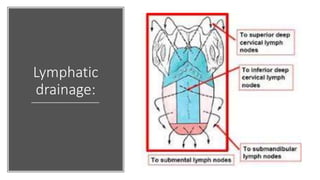
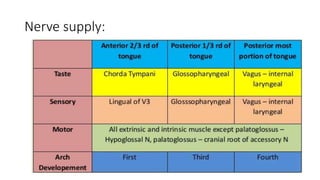
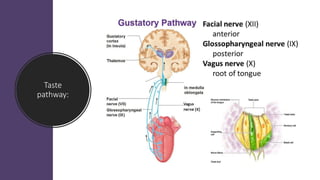
The document provides an overview of the anatomy and applied aspects of the tongue. It discusses the tongue's structure, muscles, blood supply, innervation, and development. Key points include that the tongue has extrinsic and intrinsic muscles innervated by the hypoglossal nerve and is supplied by the lingual artery. The tongue contains various papillae and serves roles in taste, swallowing, and speech. Applied aspects discussed include injuries, tumors, infections, and developmental abnormalities that can affect the tongue's function and structure.