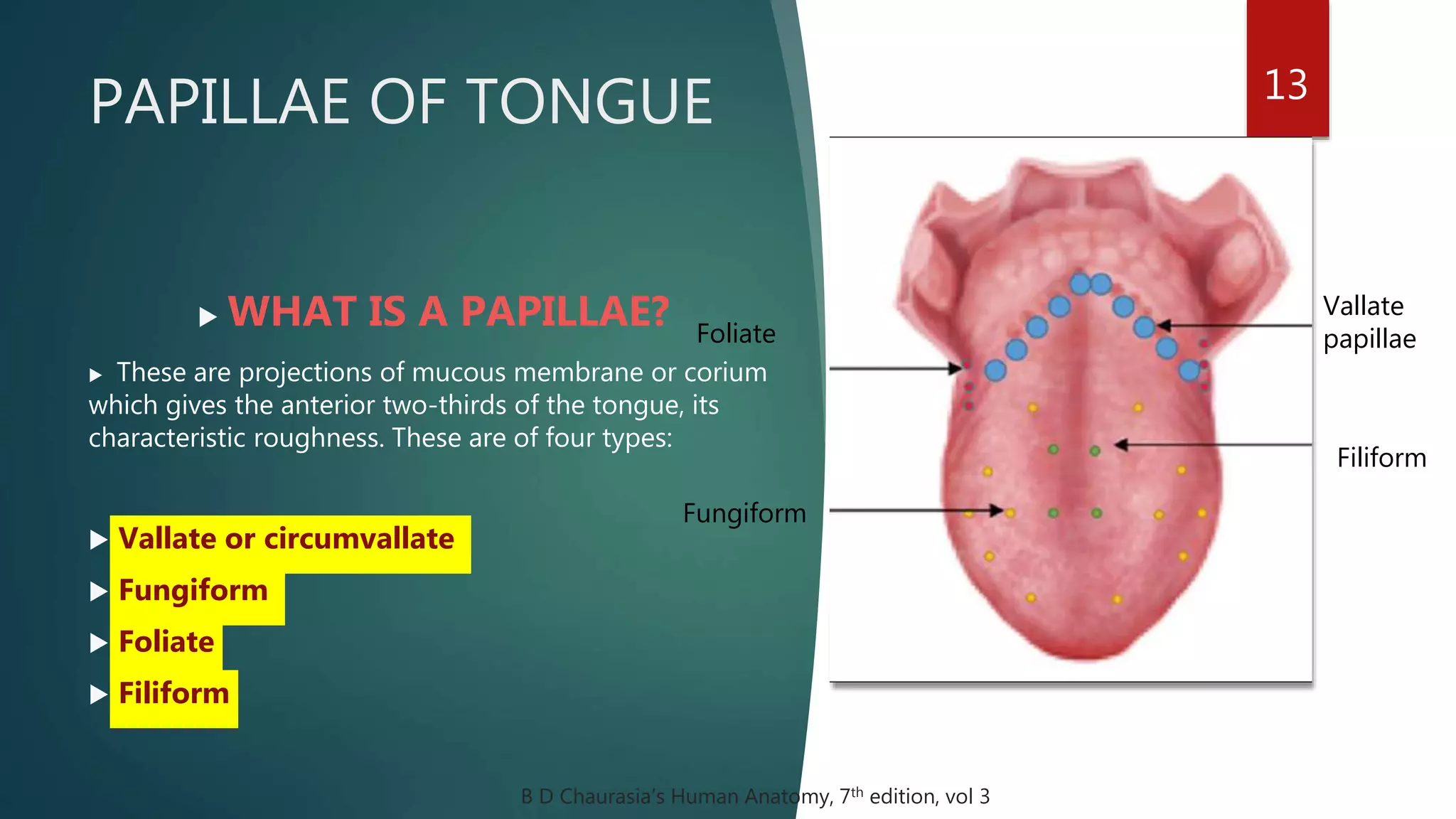
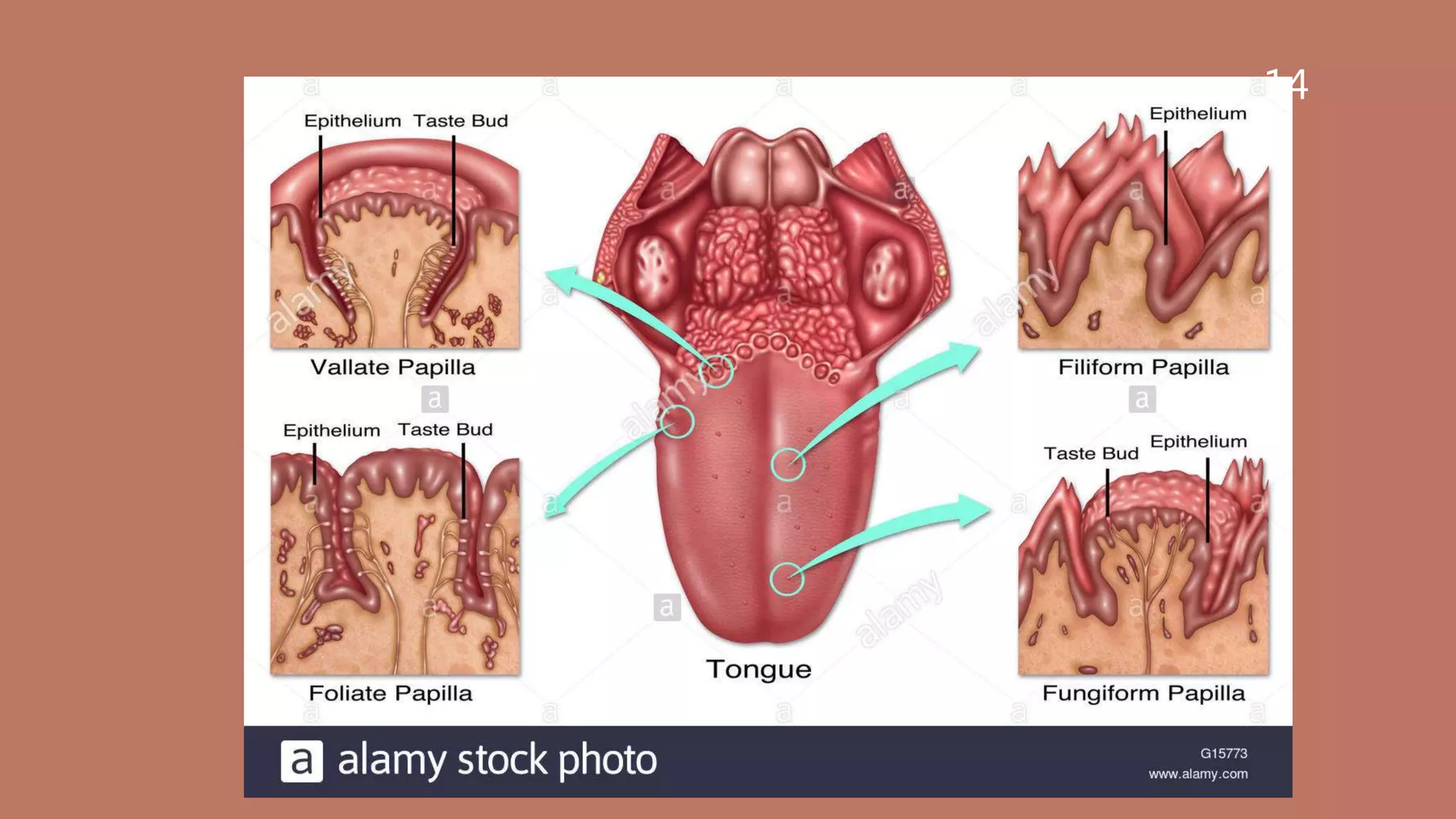
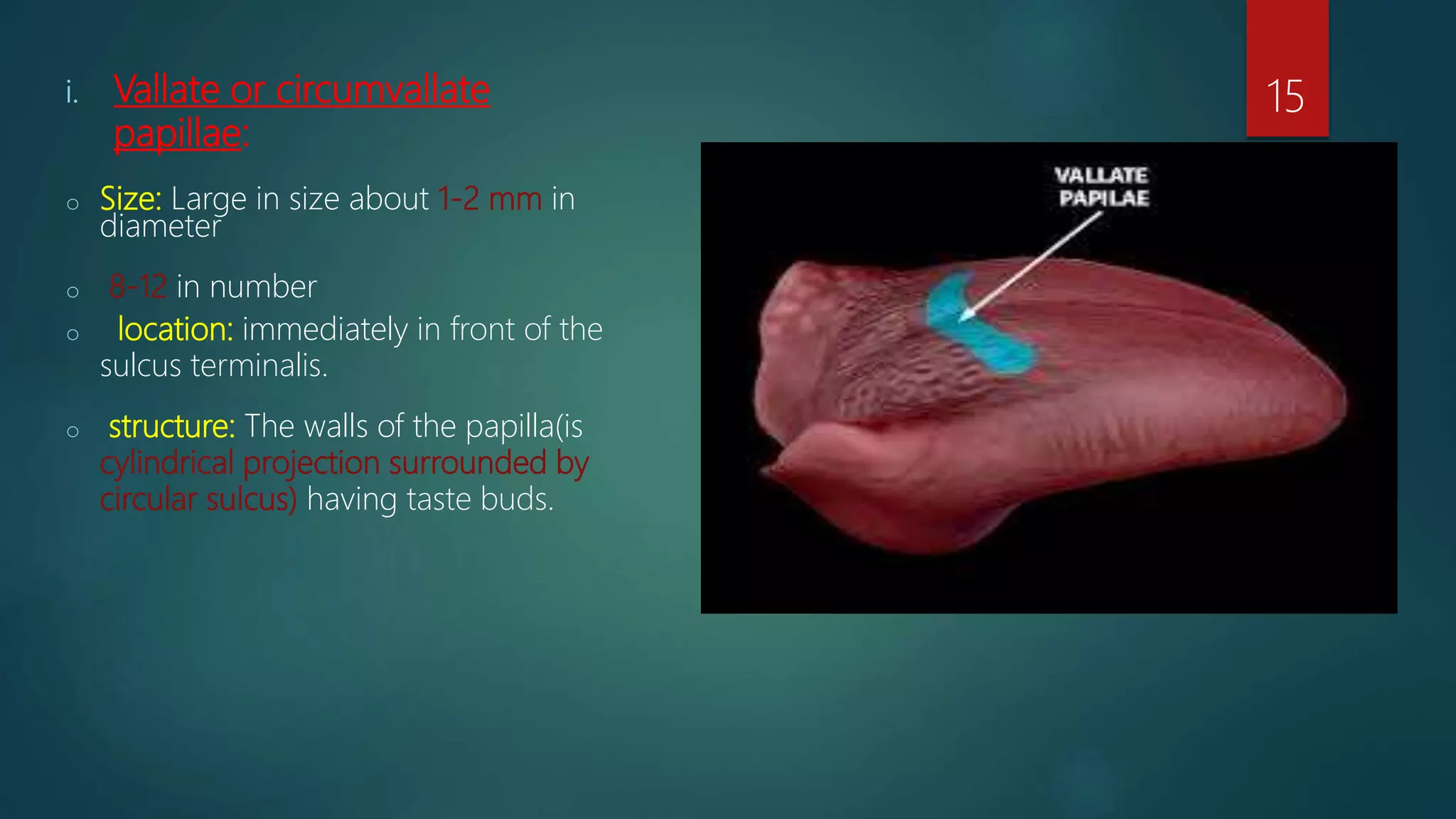
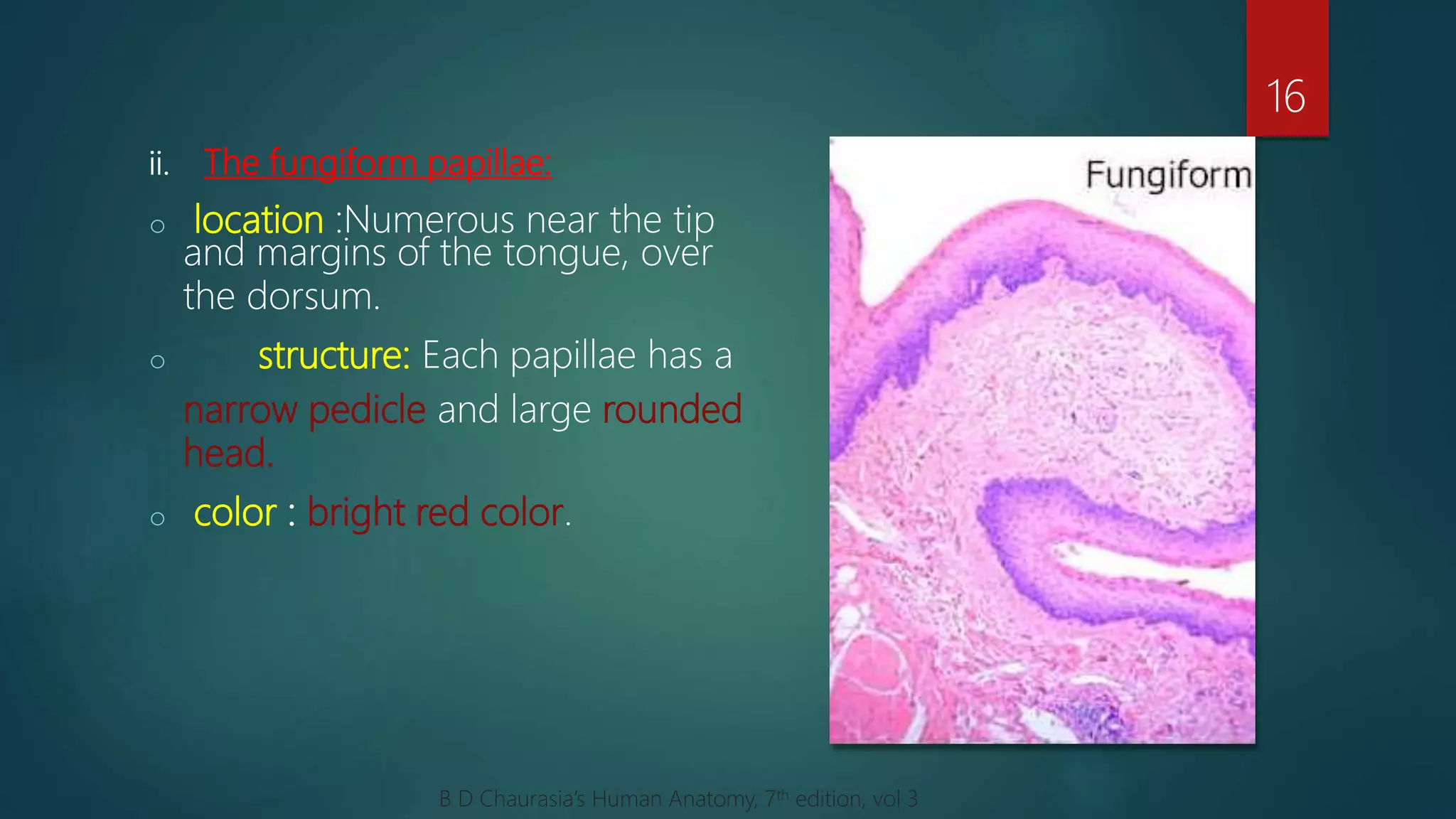
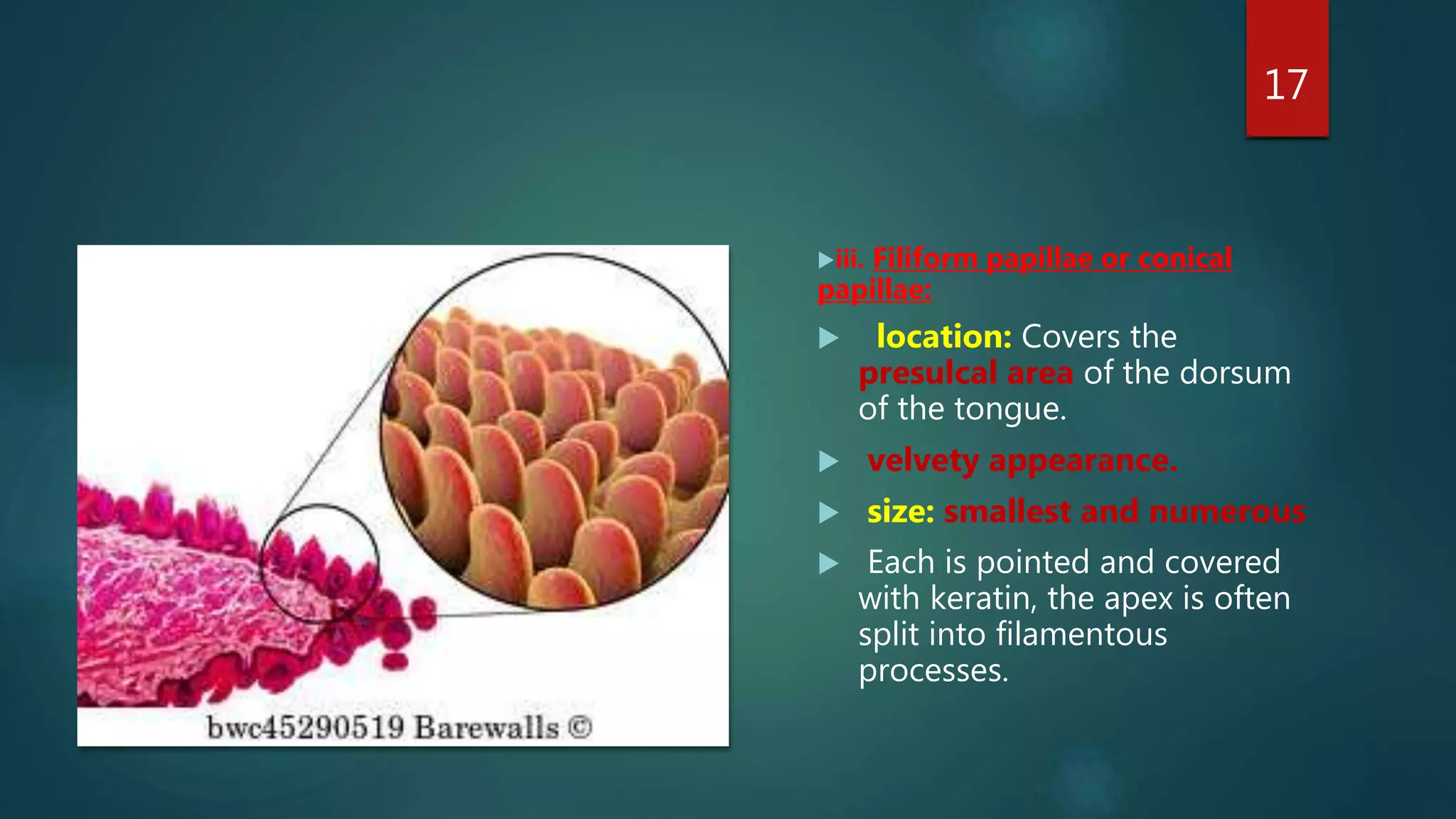
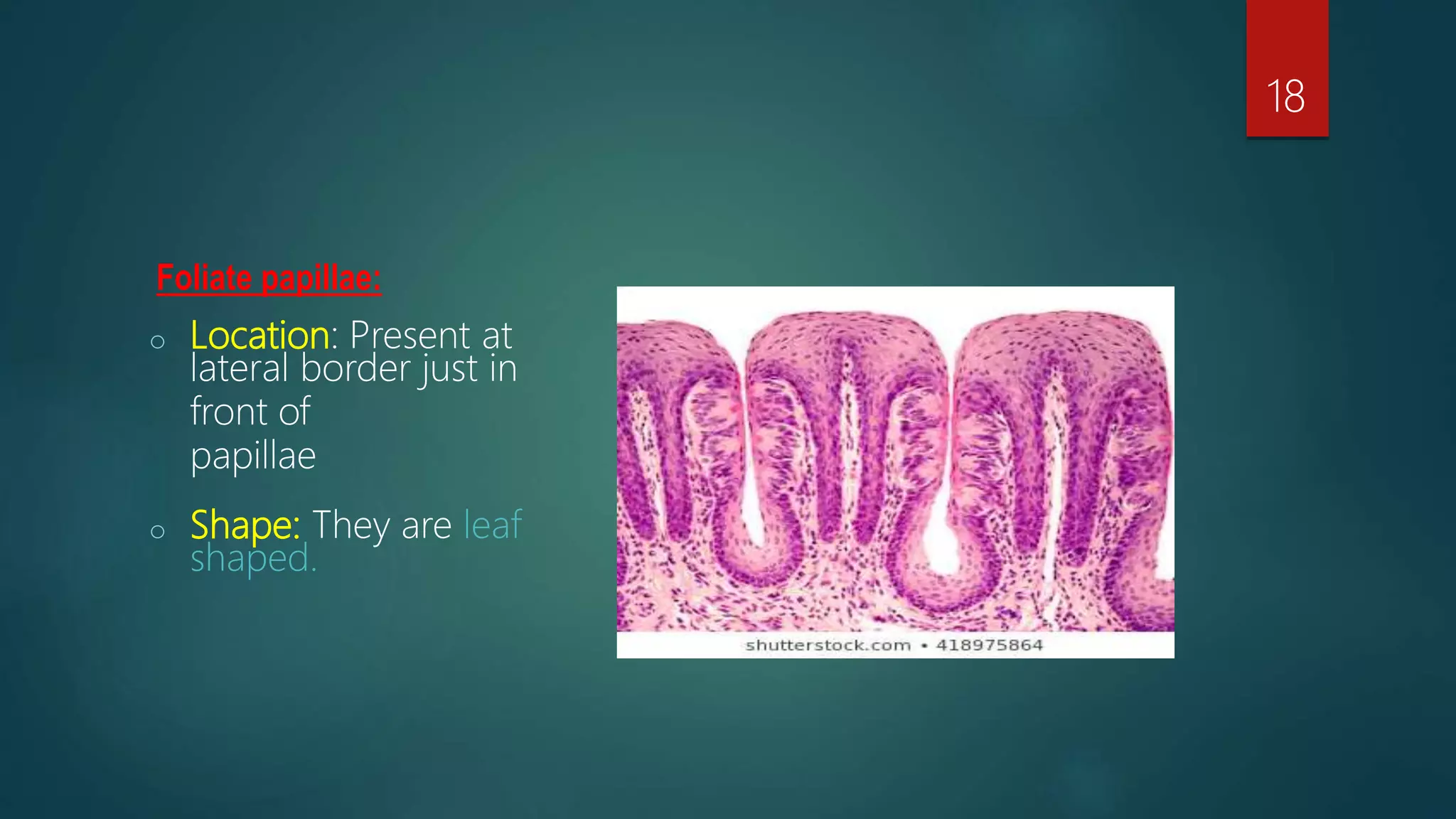
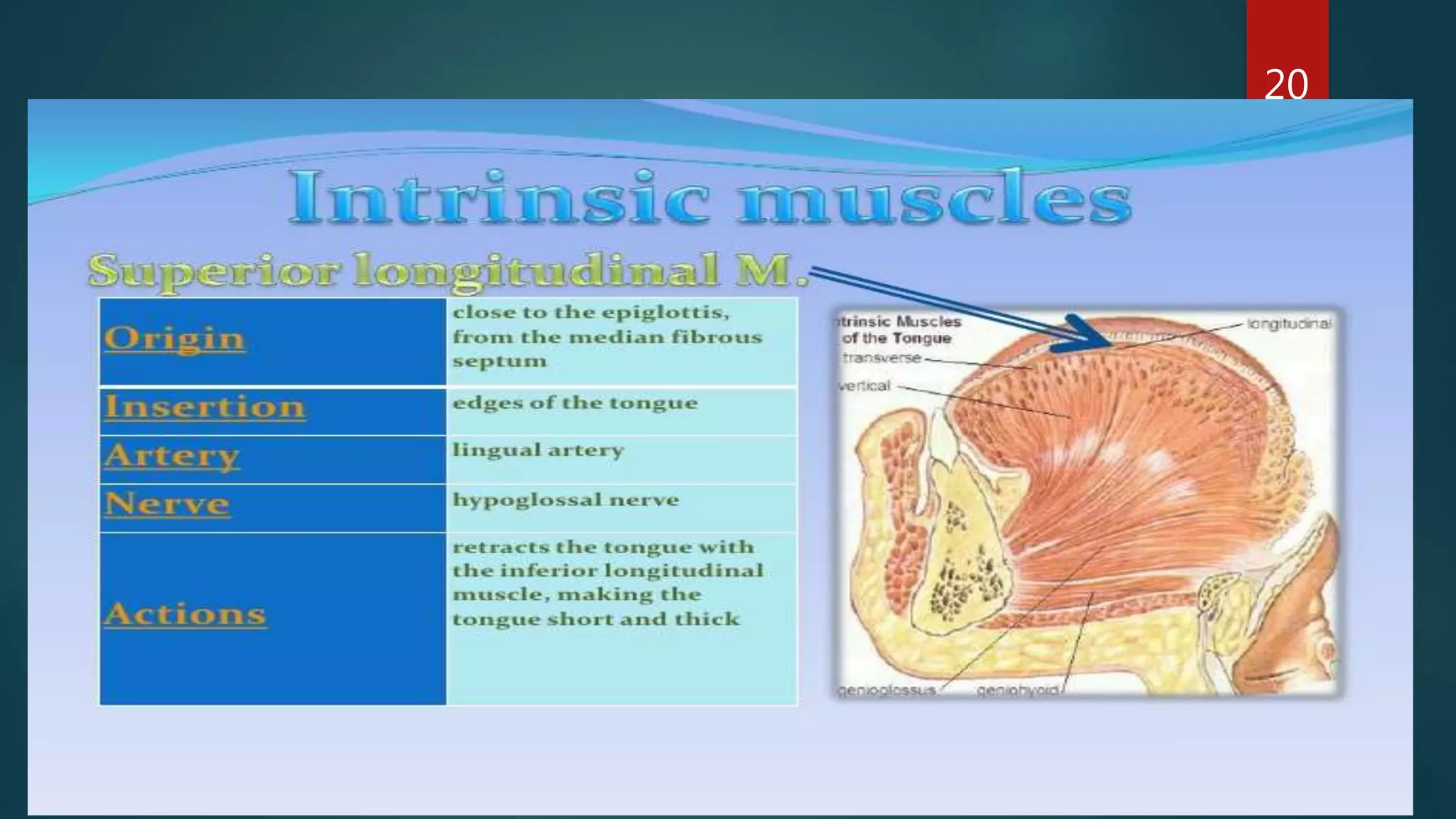
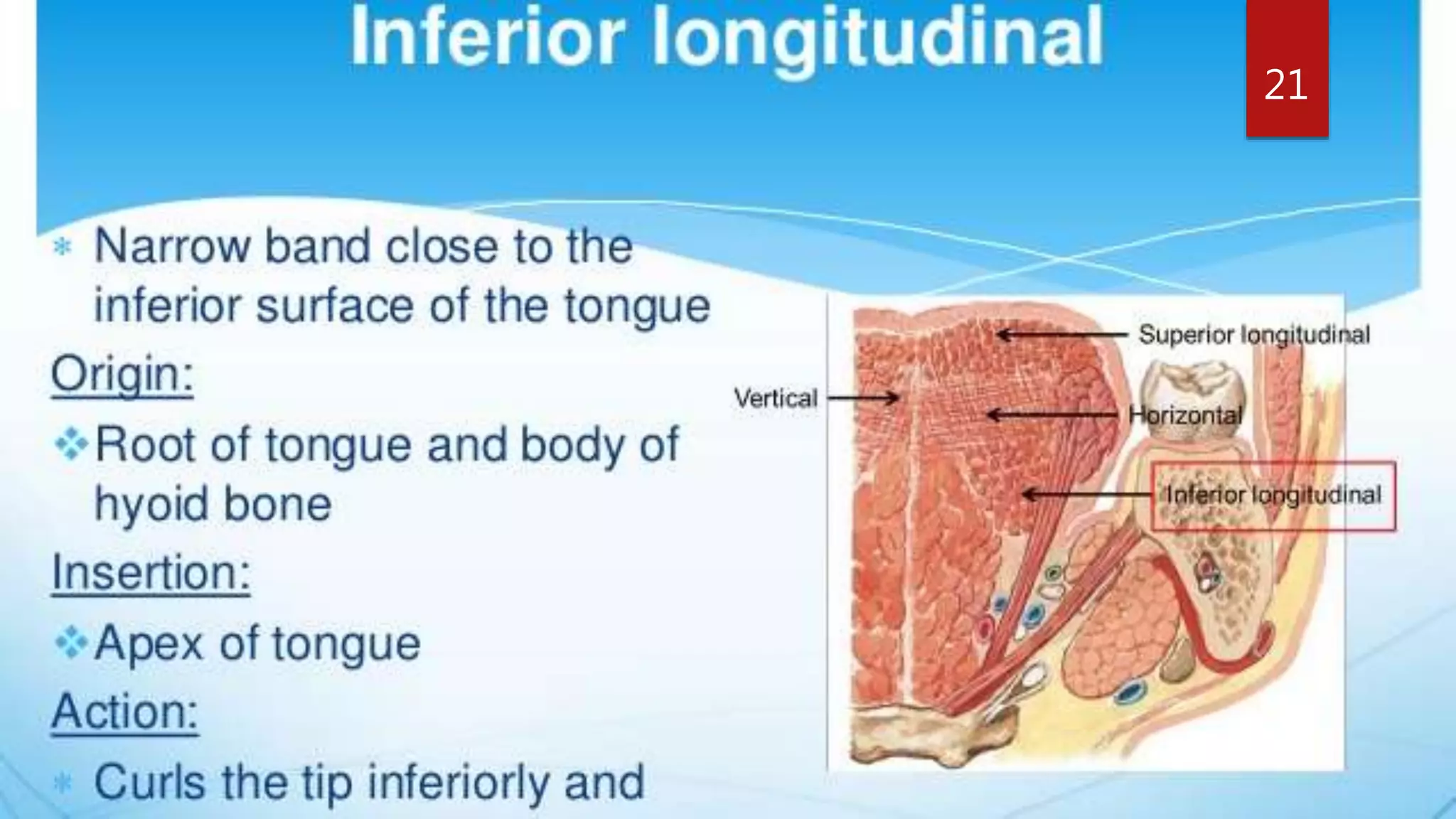
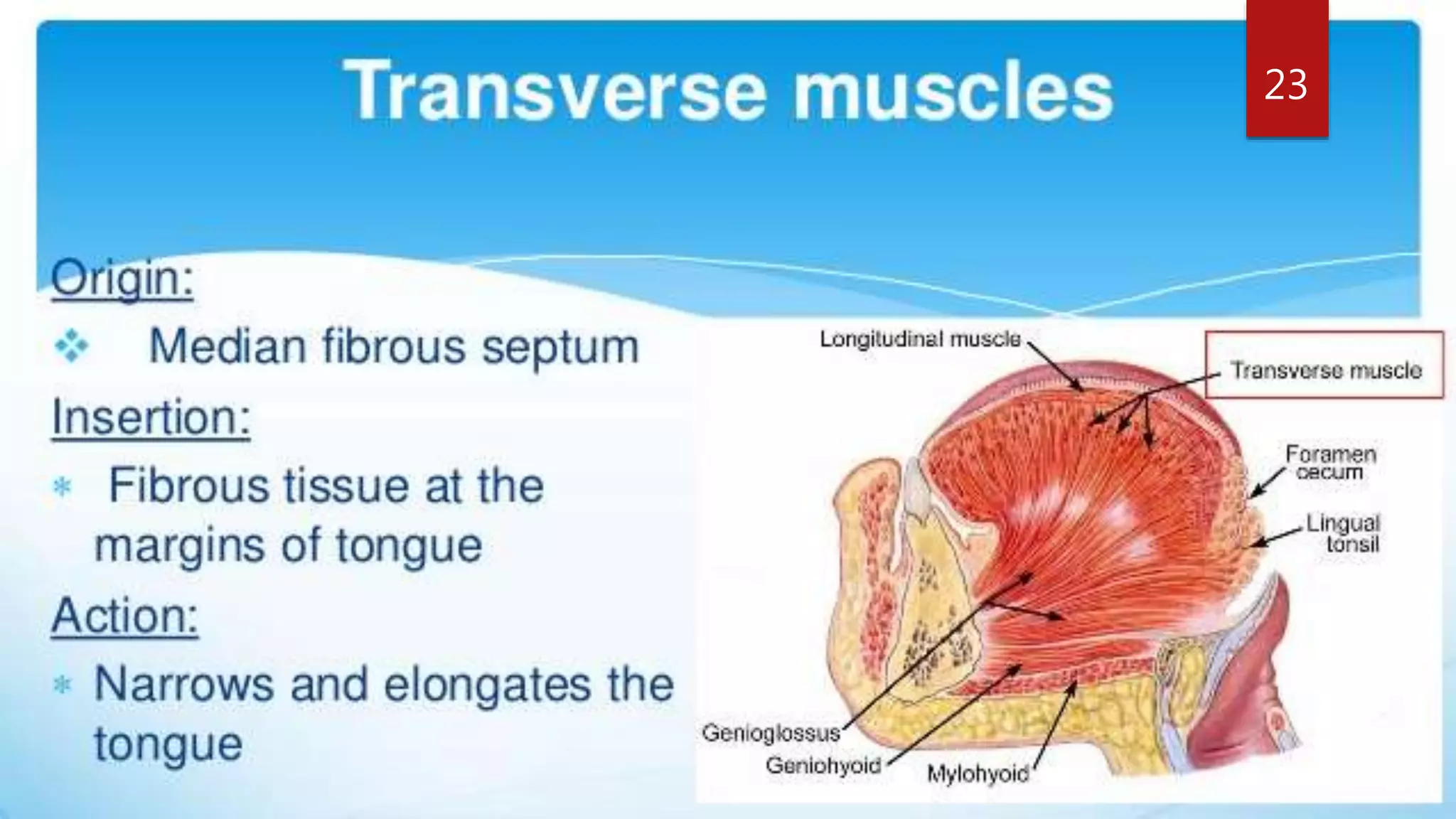
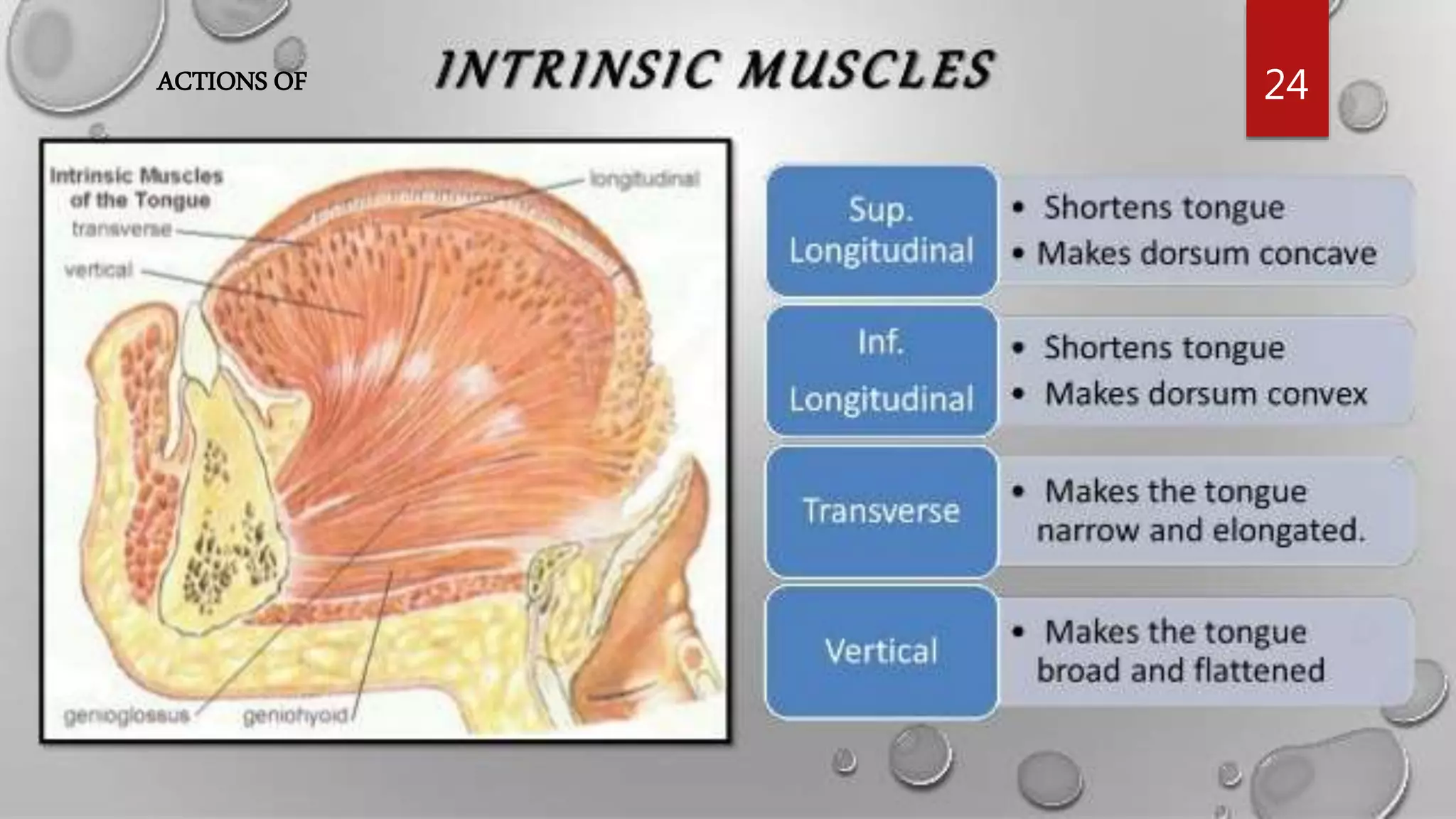
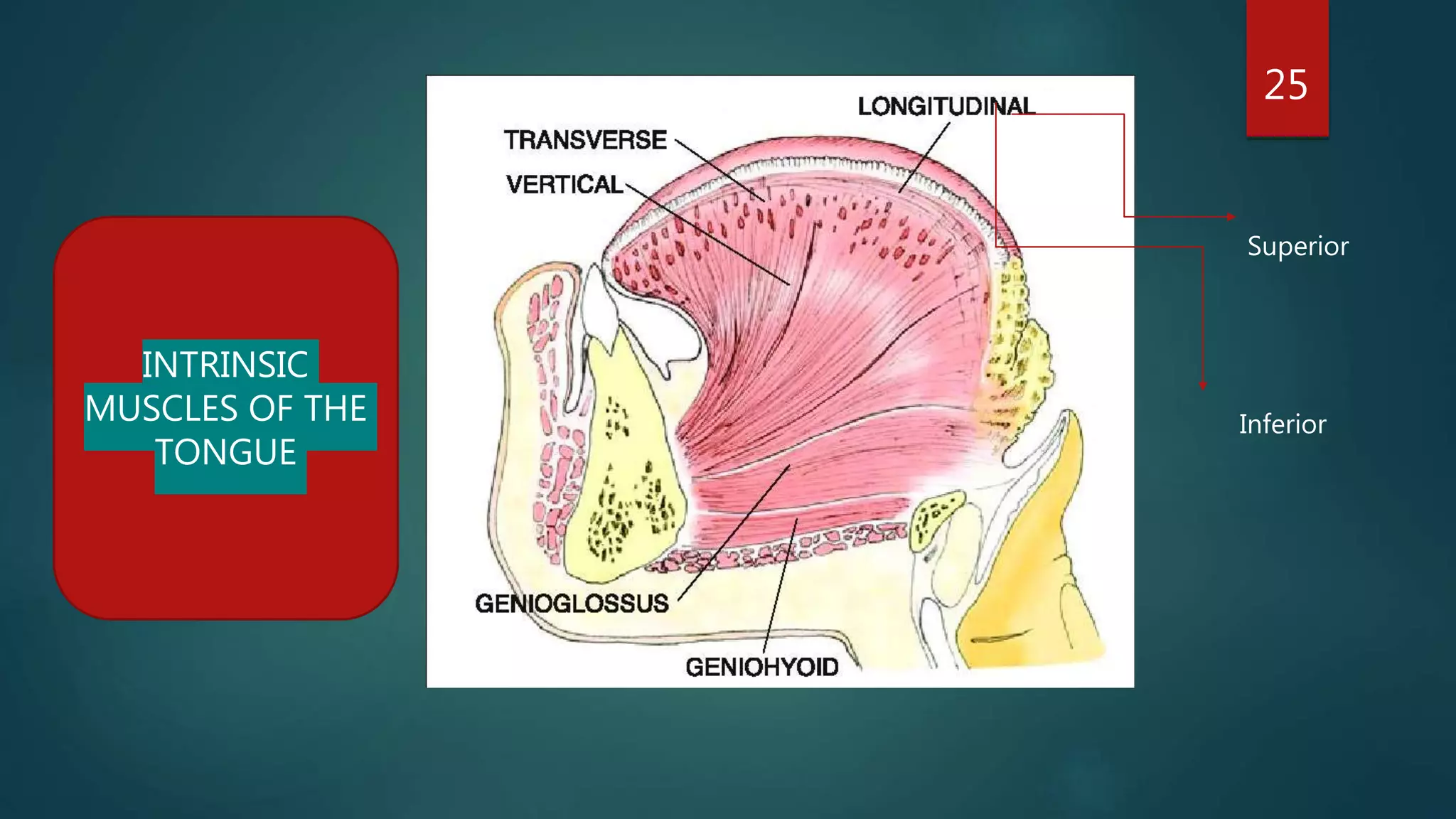
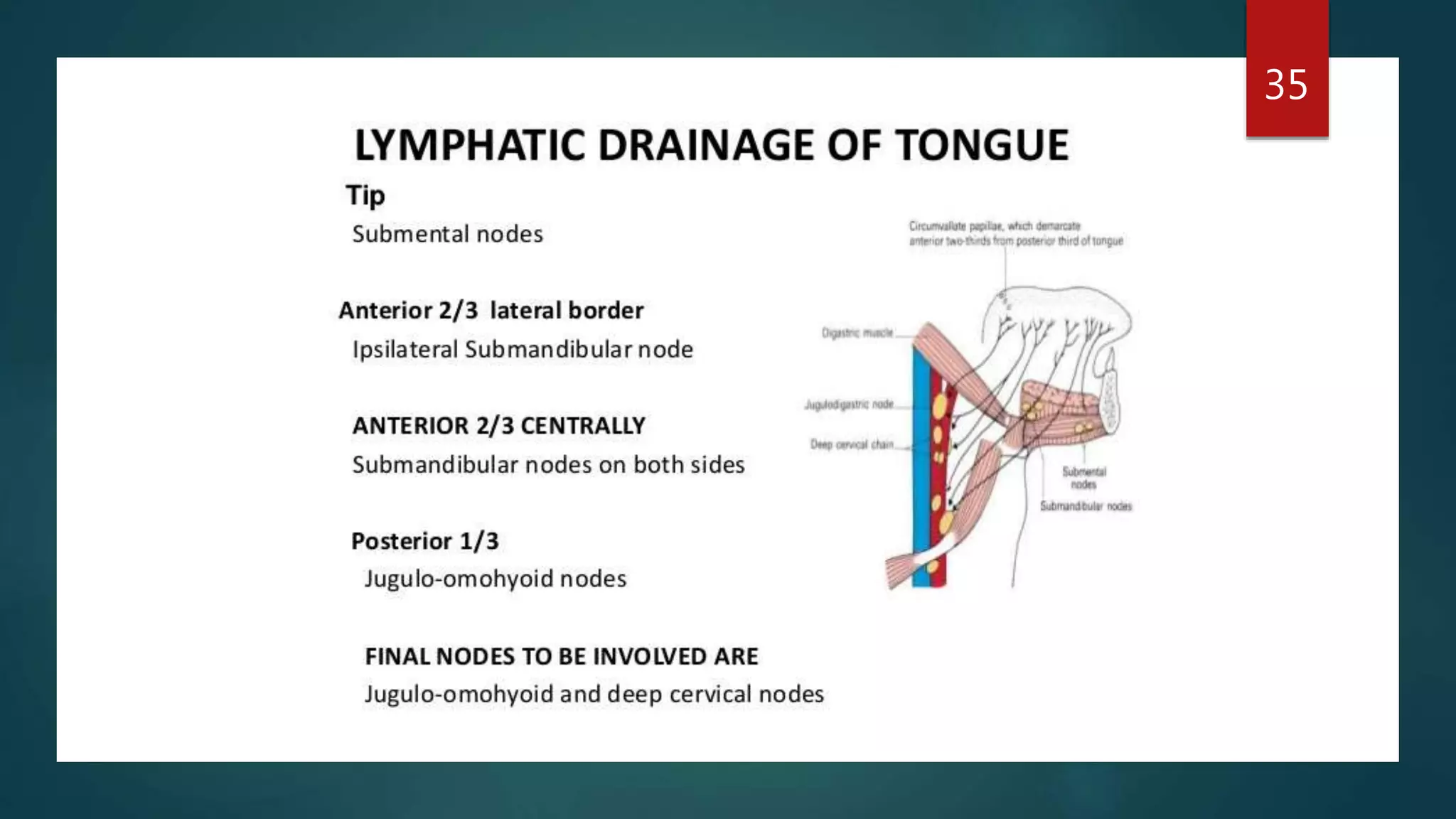
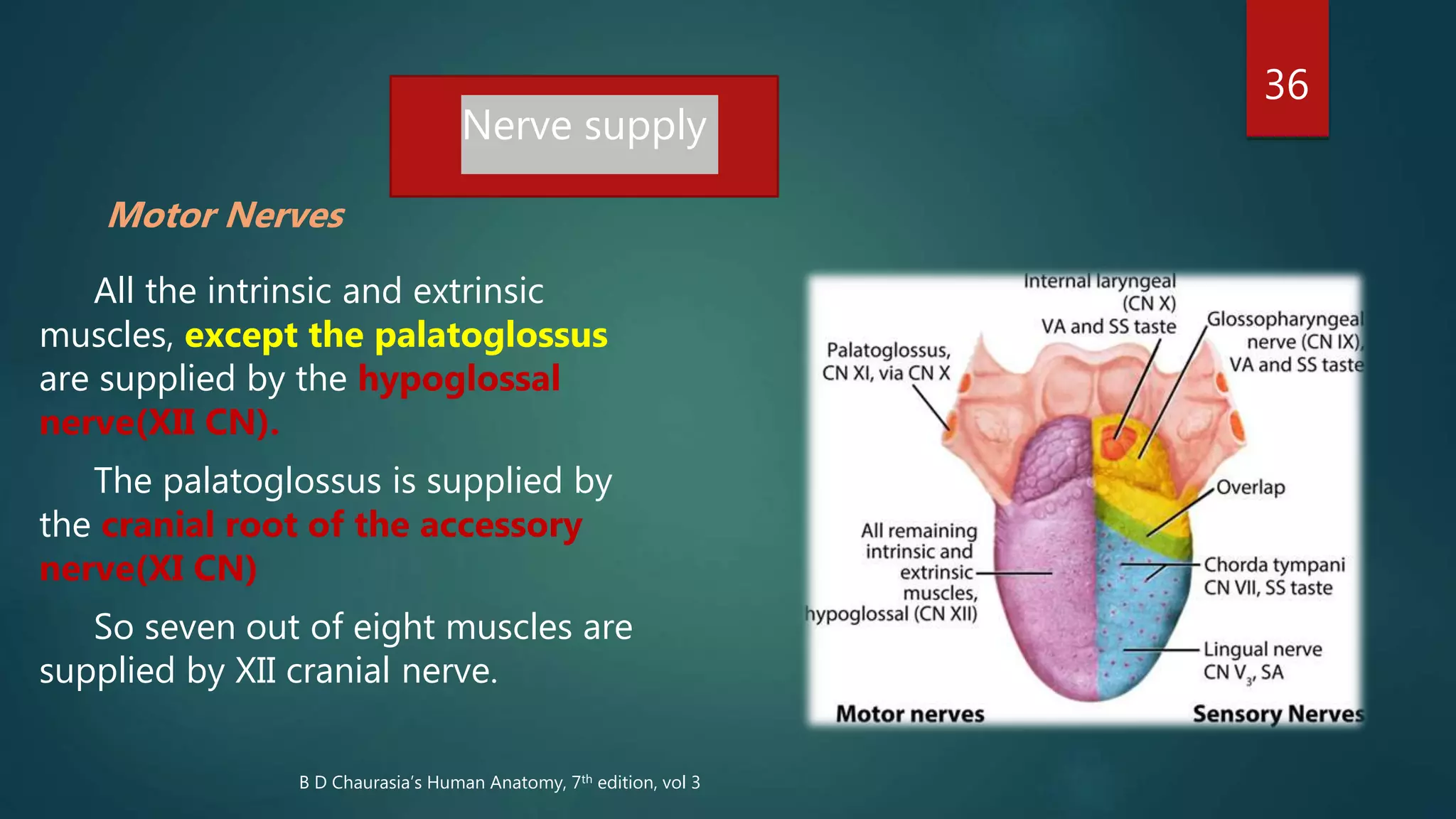
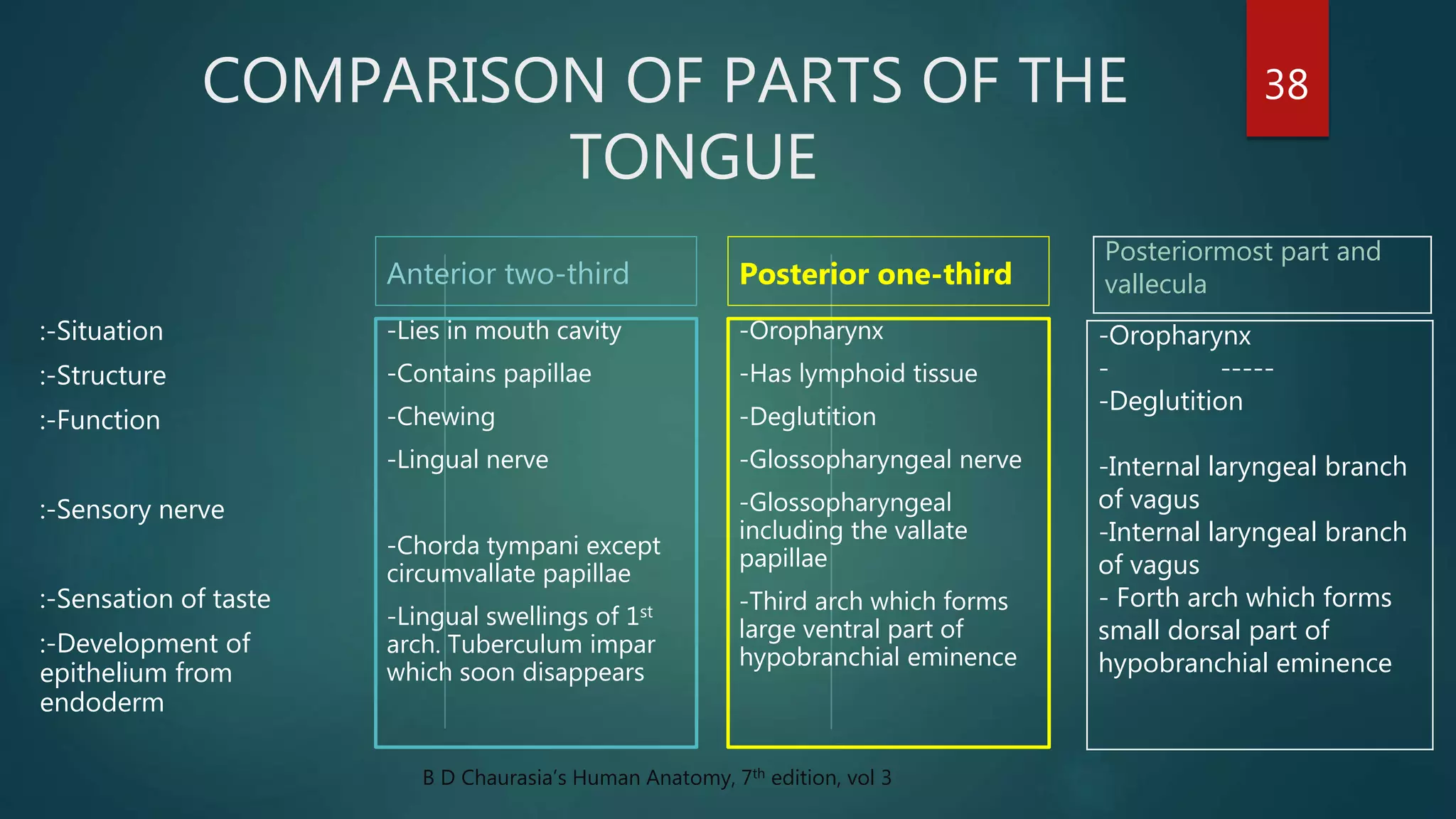
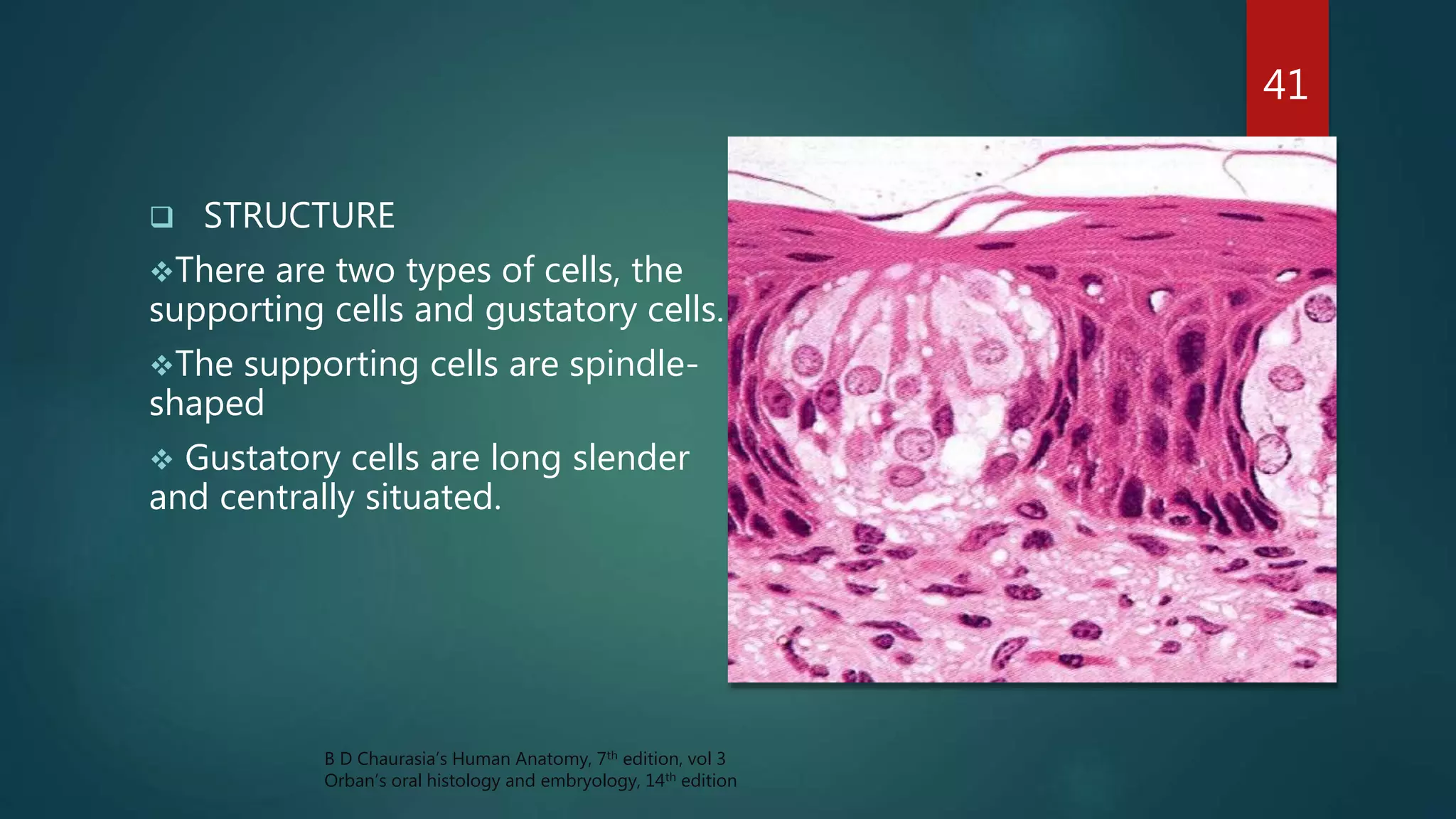
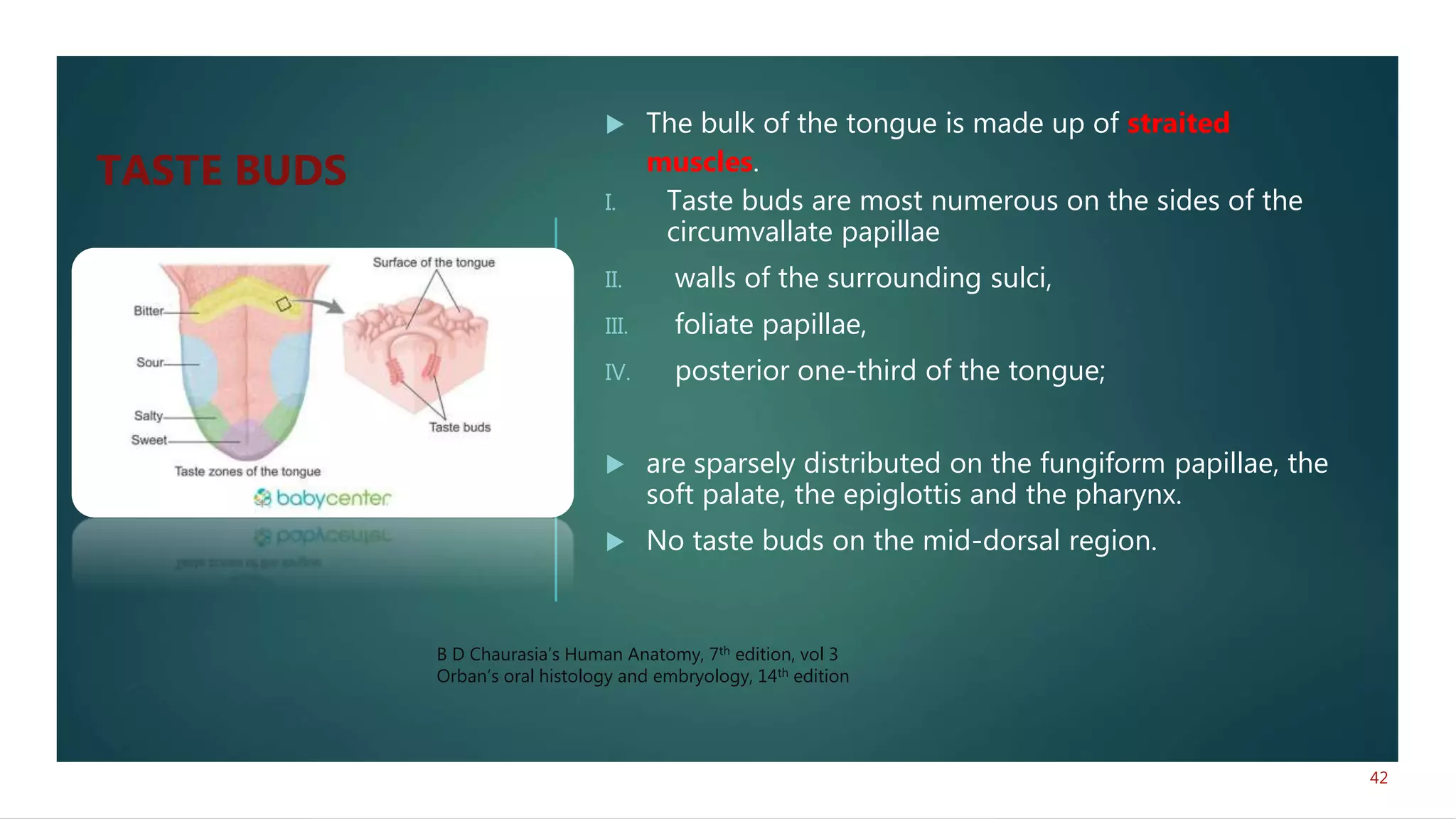
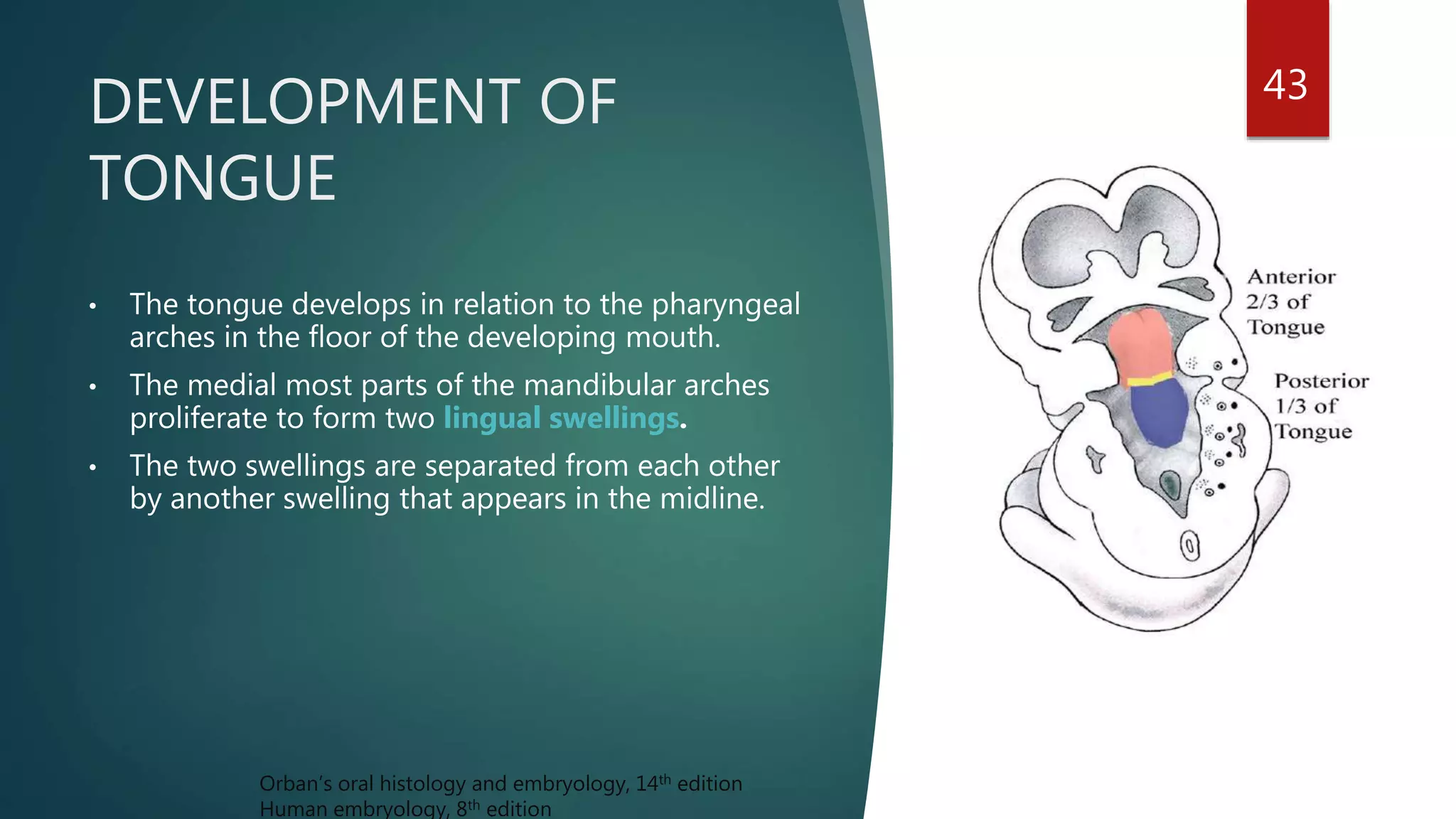
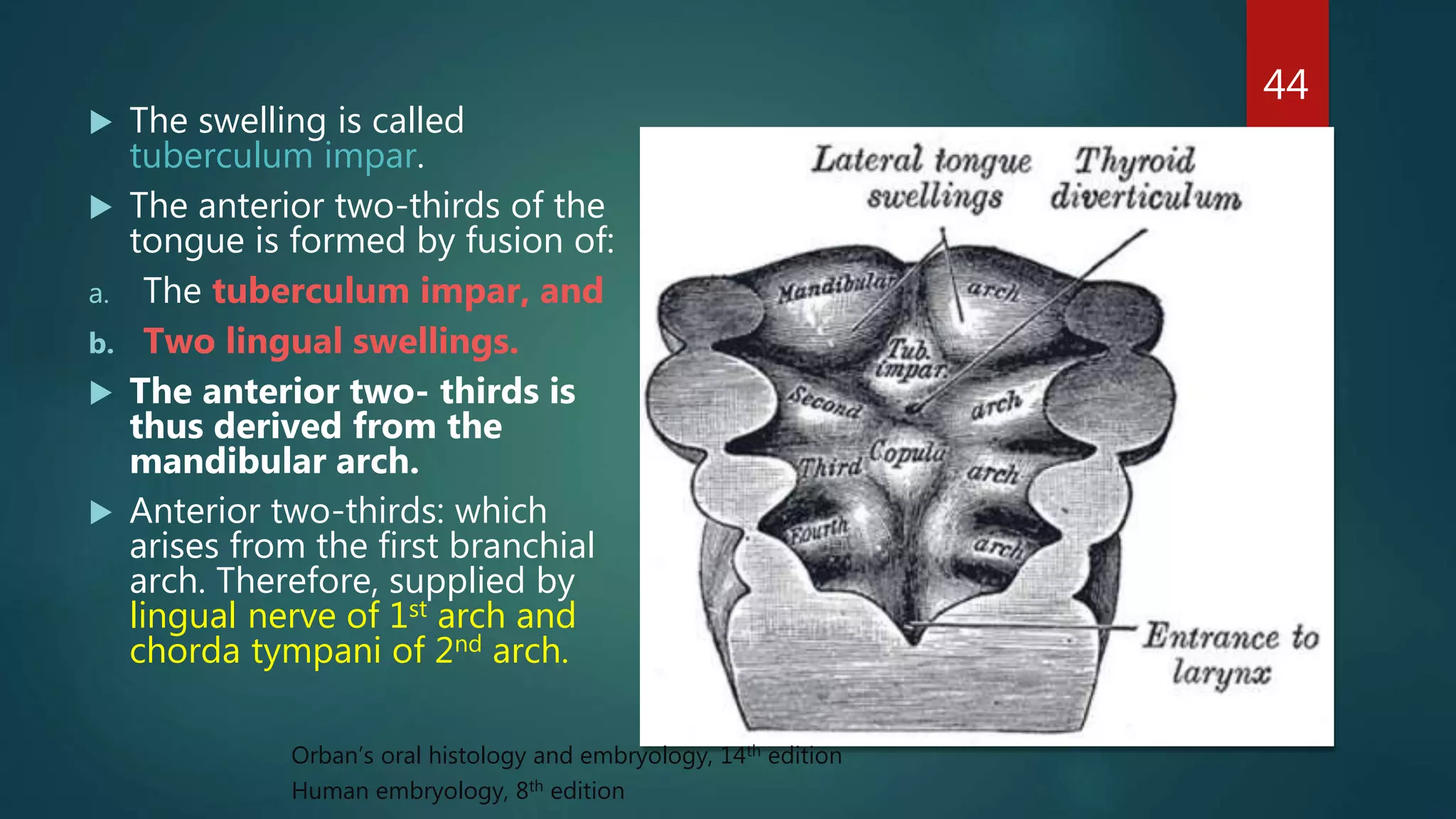
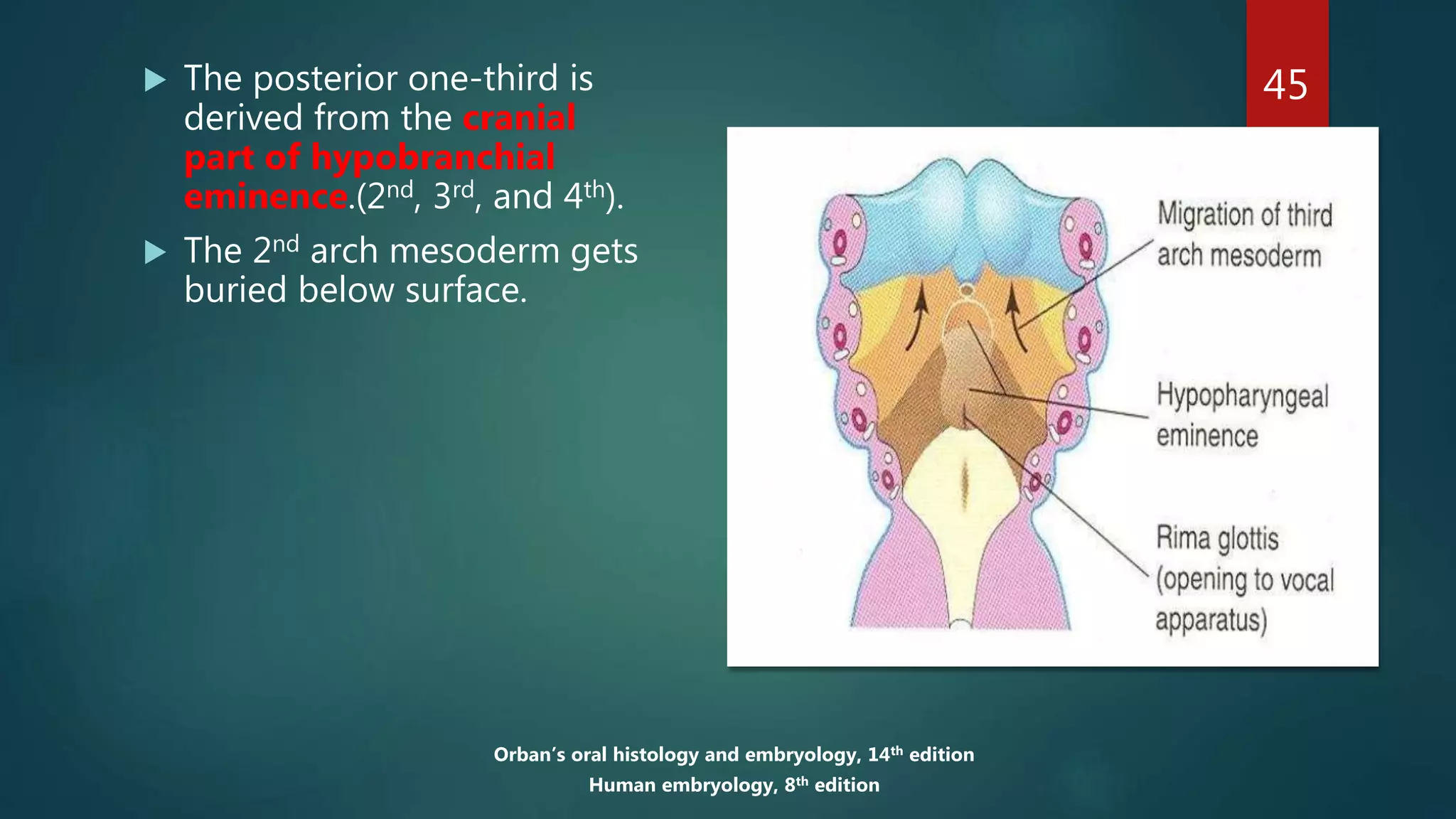
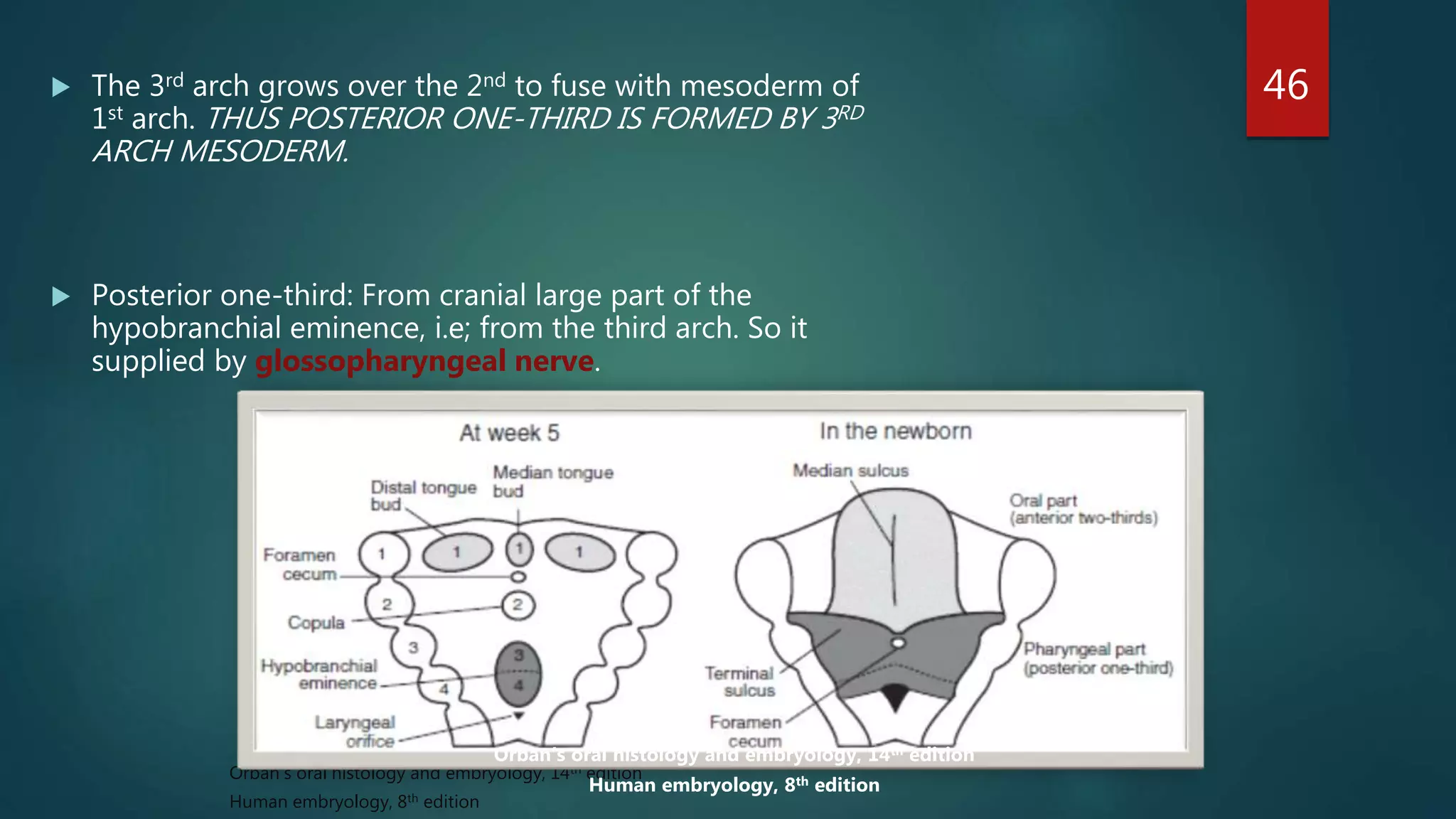
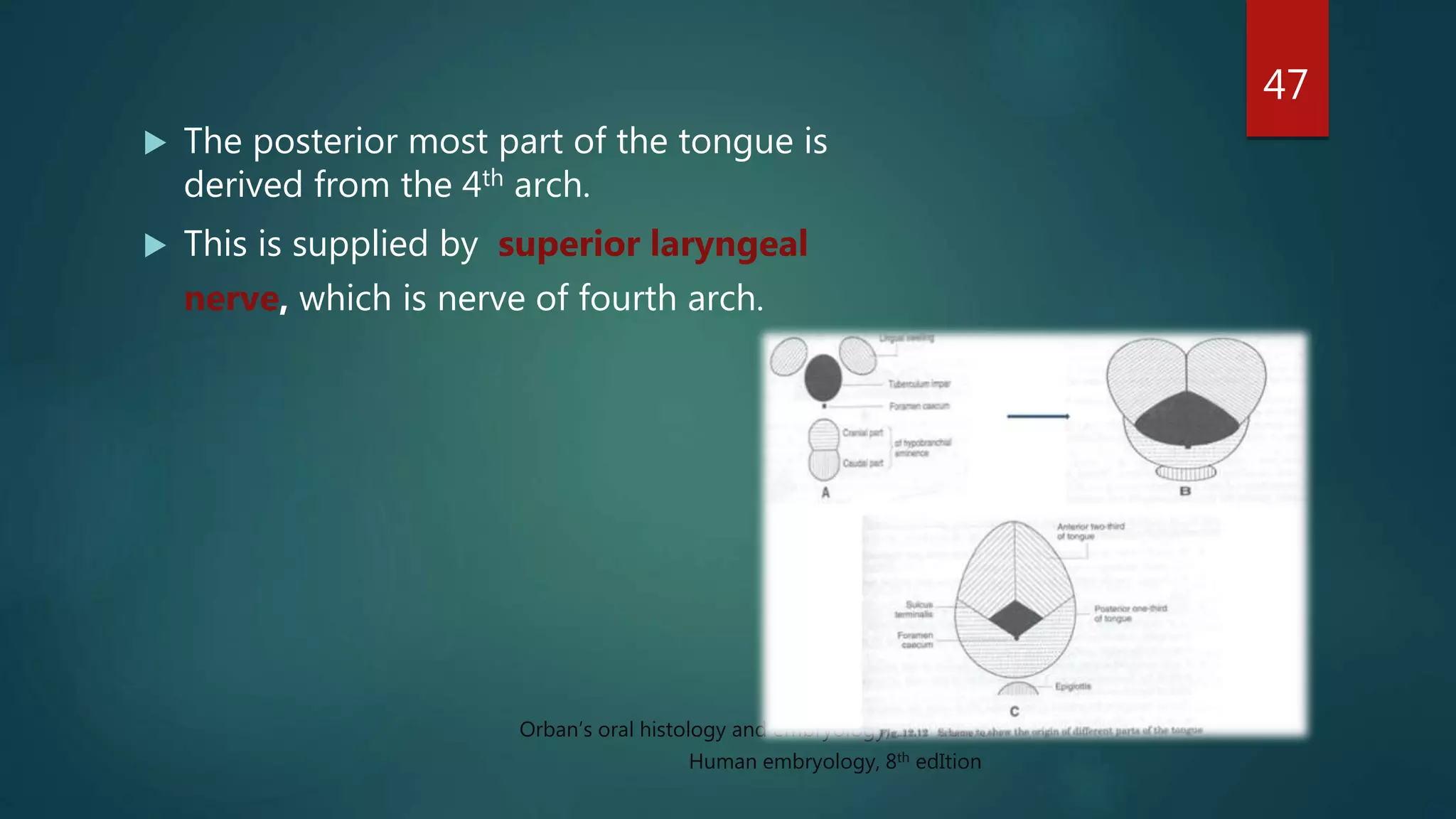
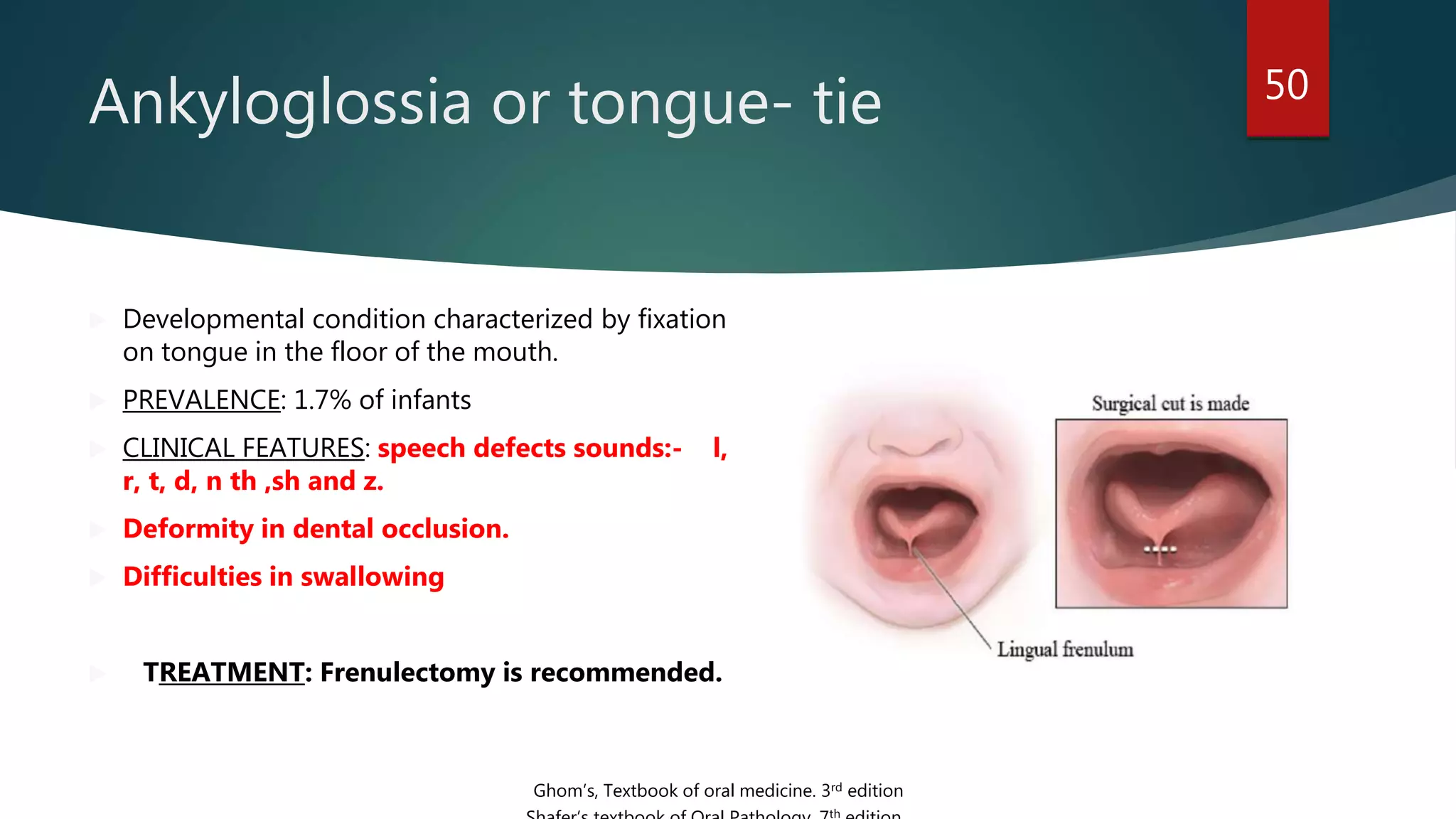
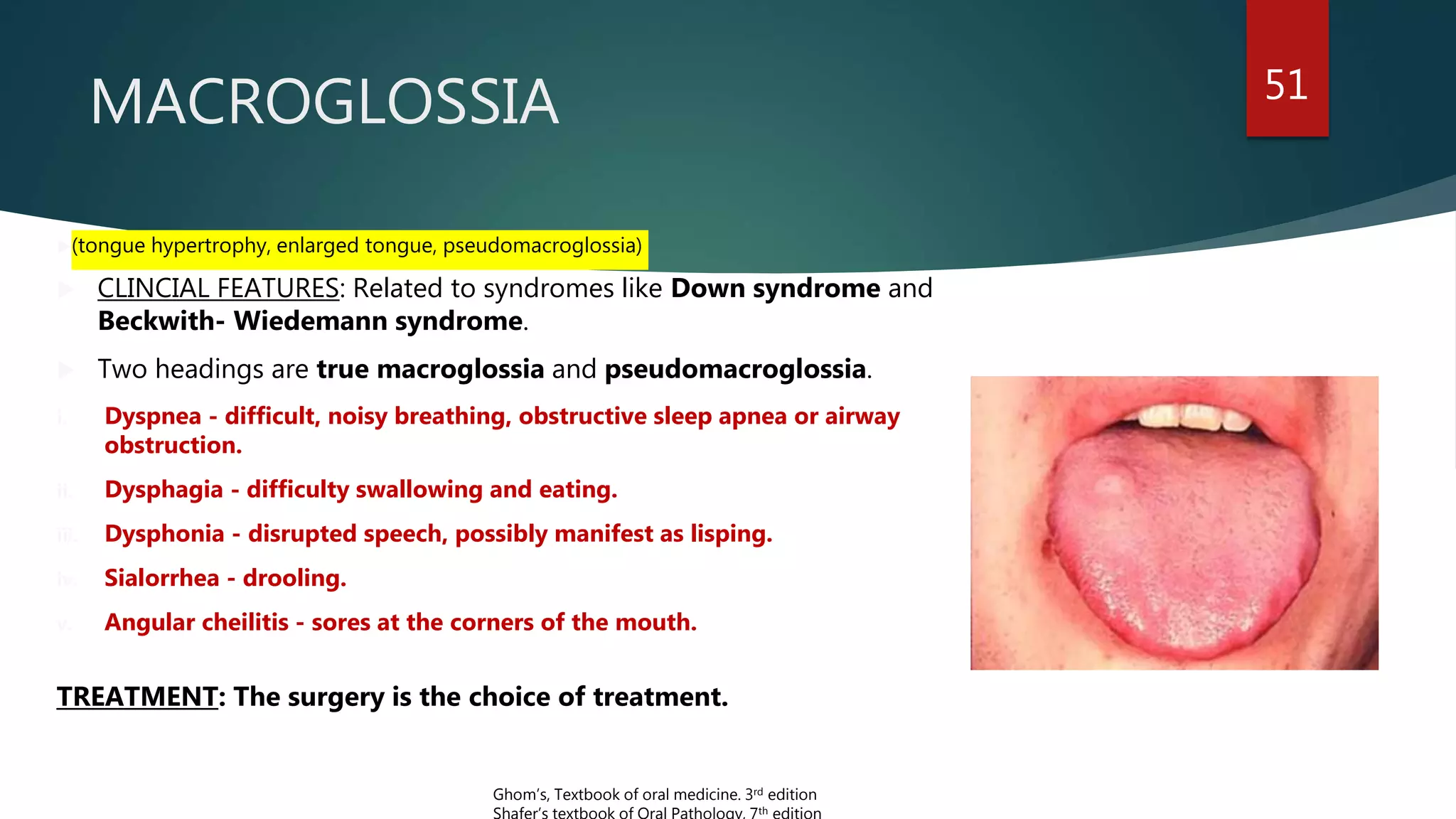
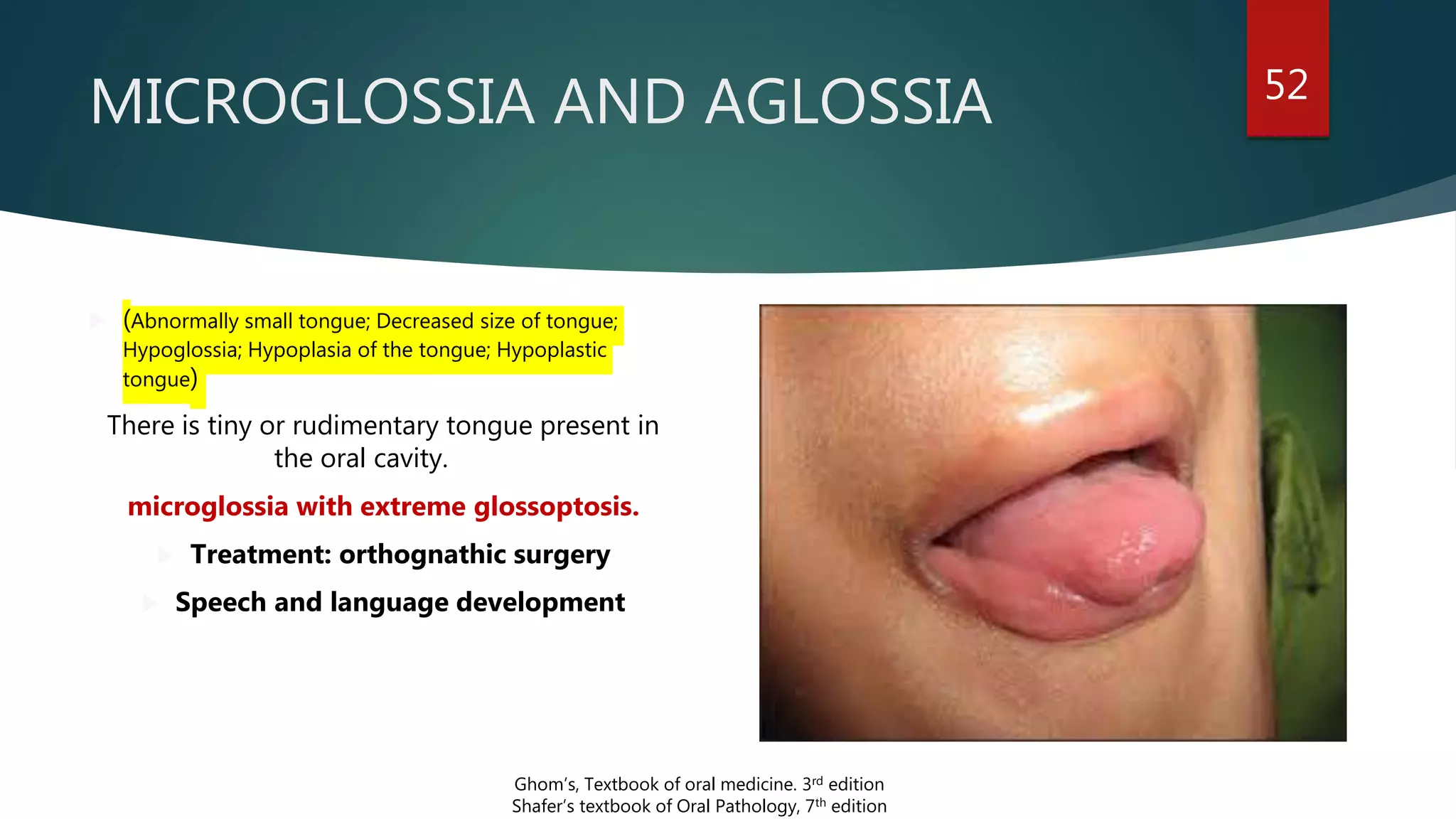
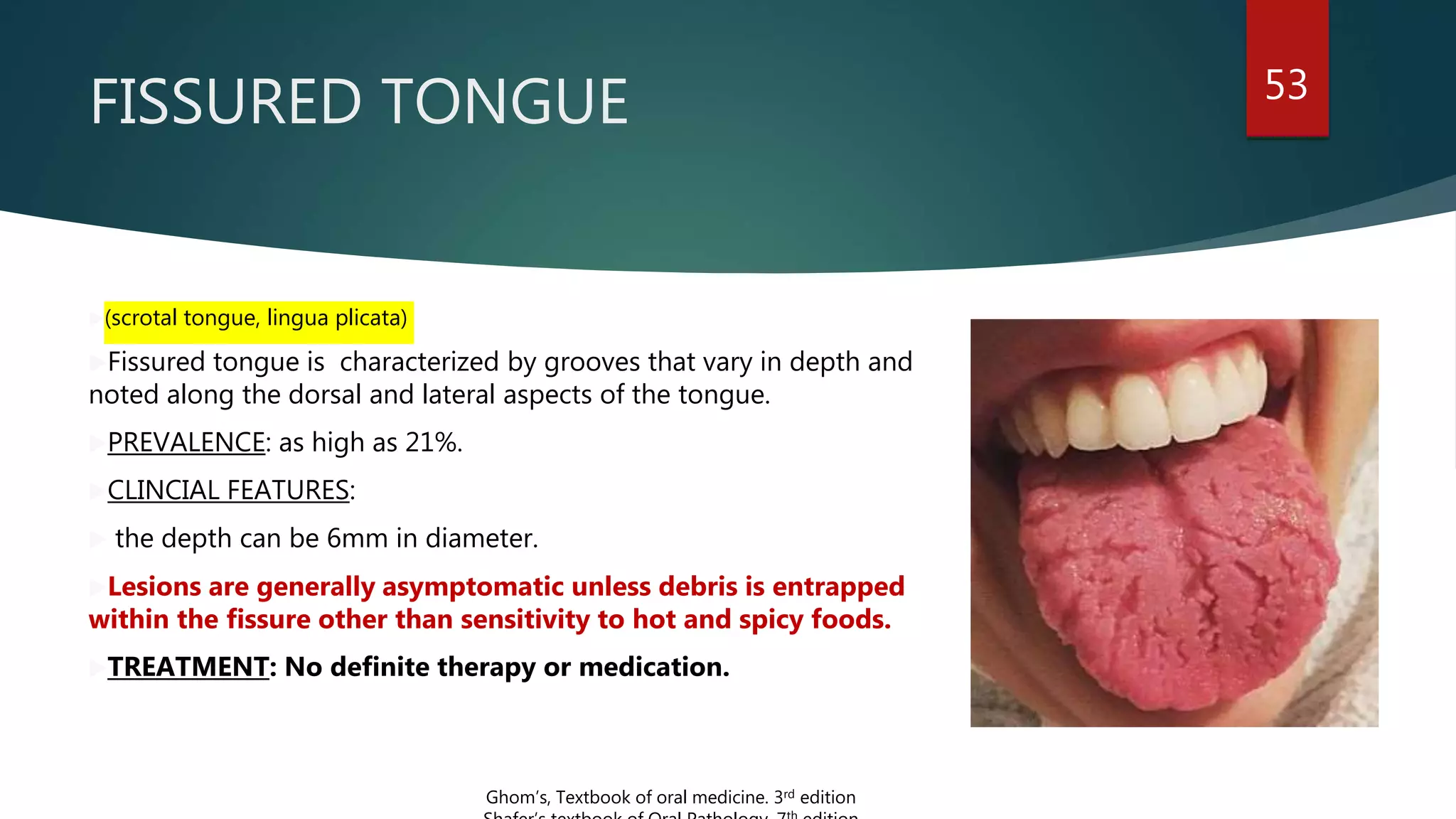
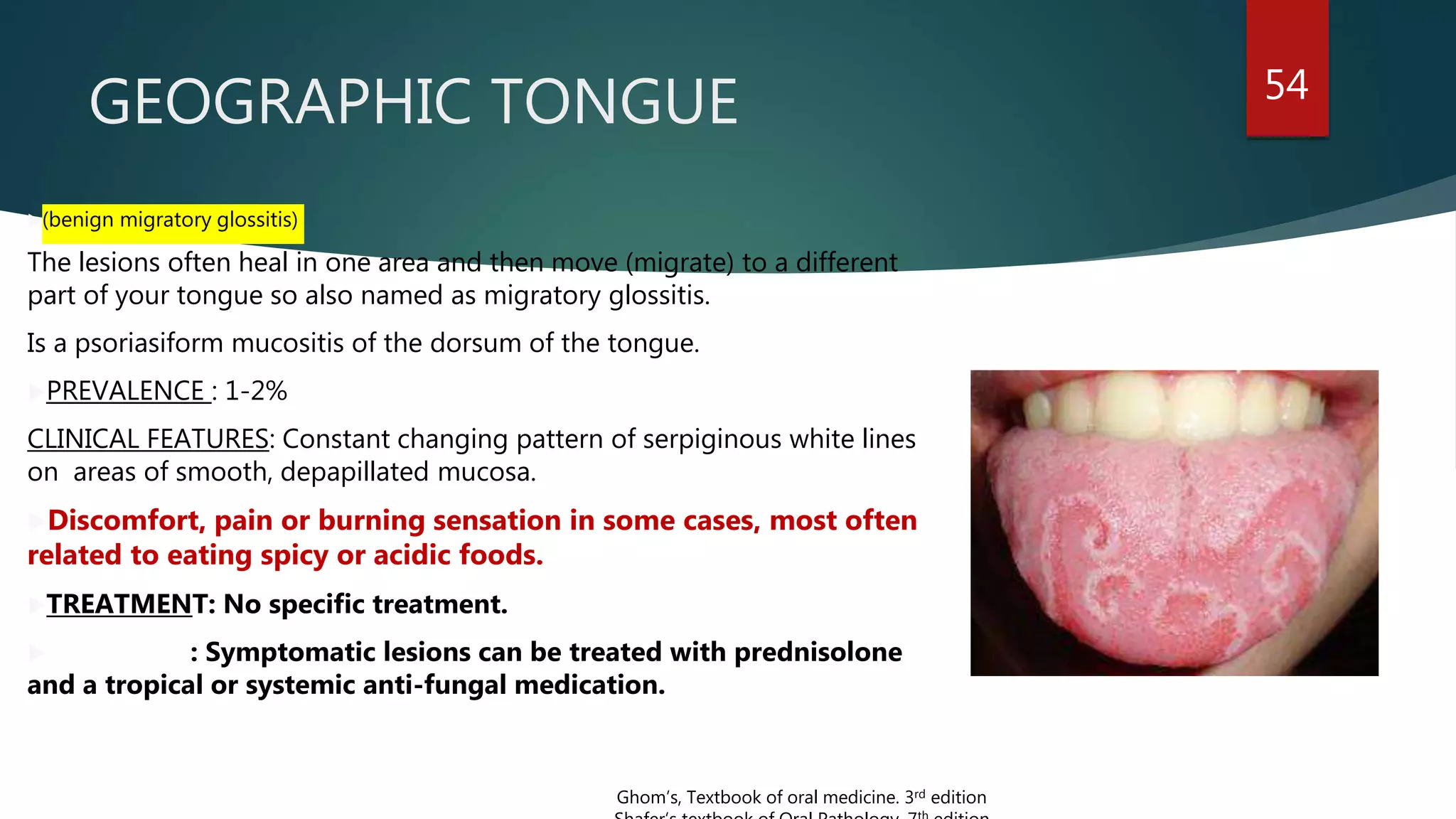
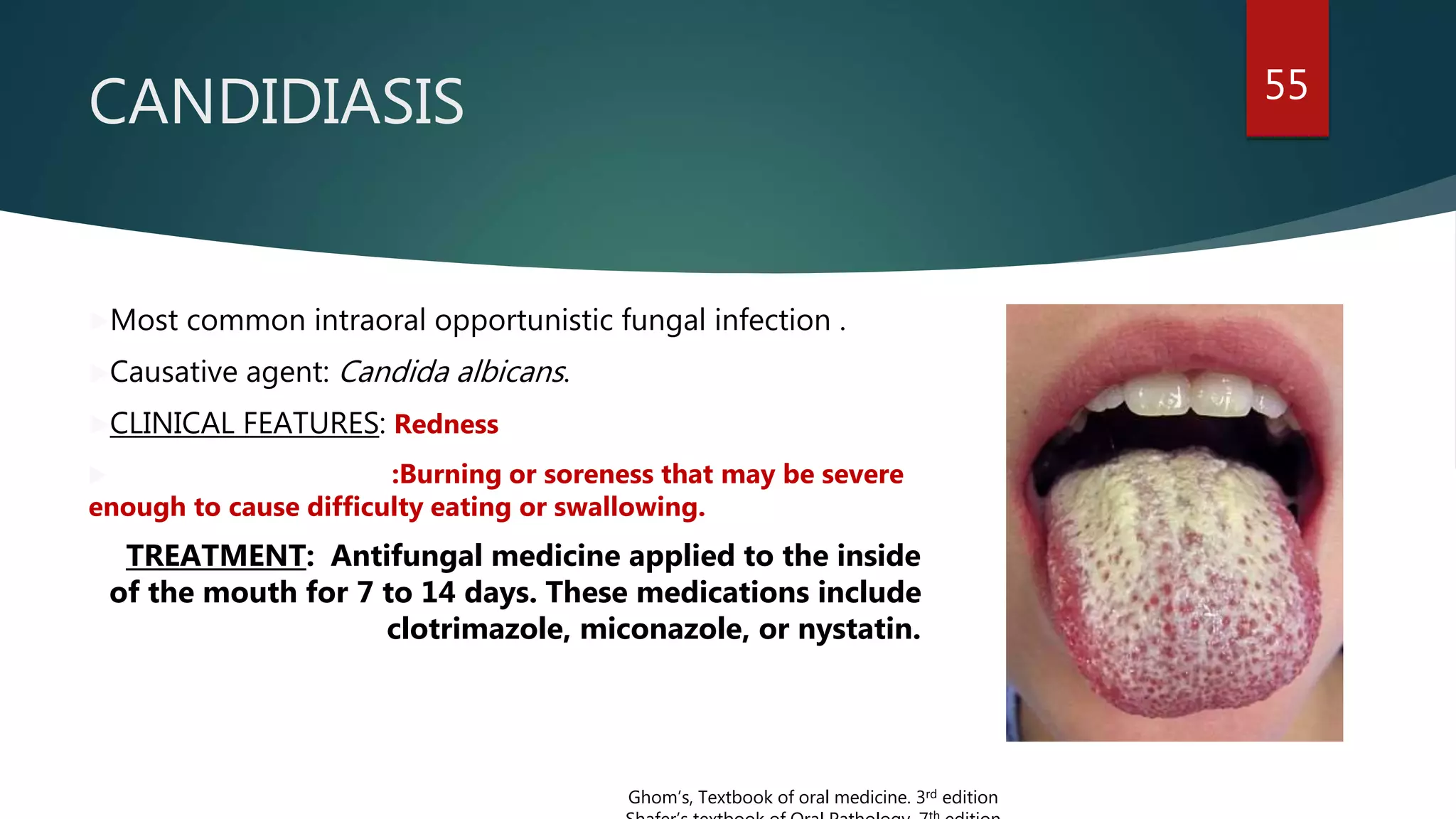
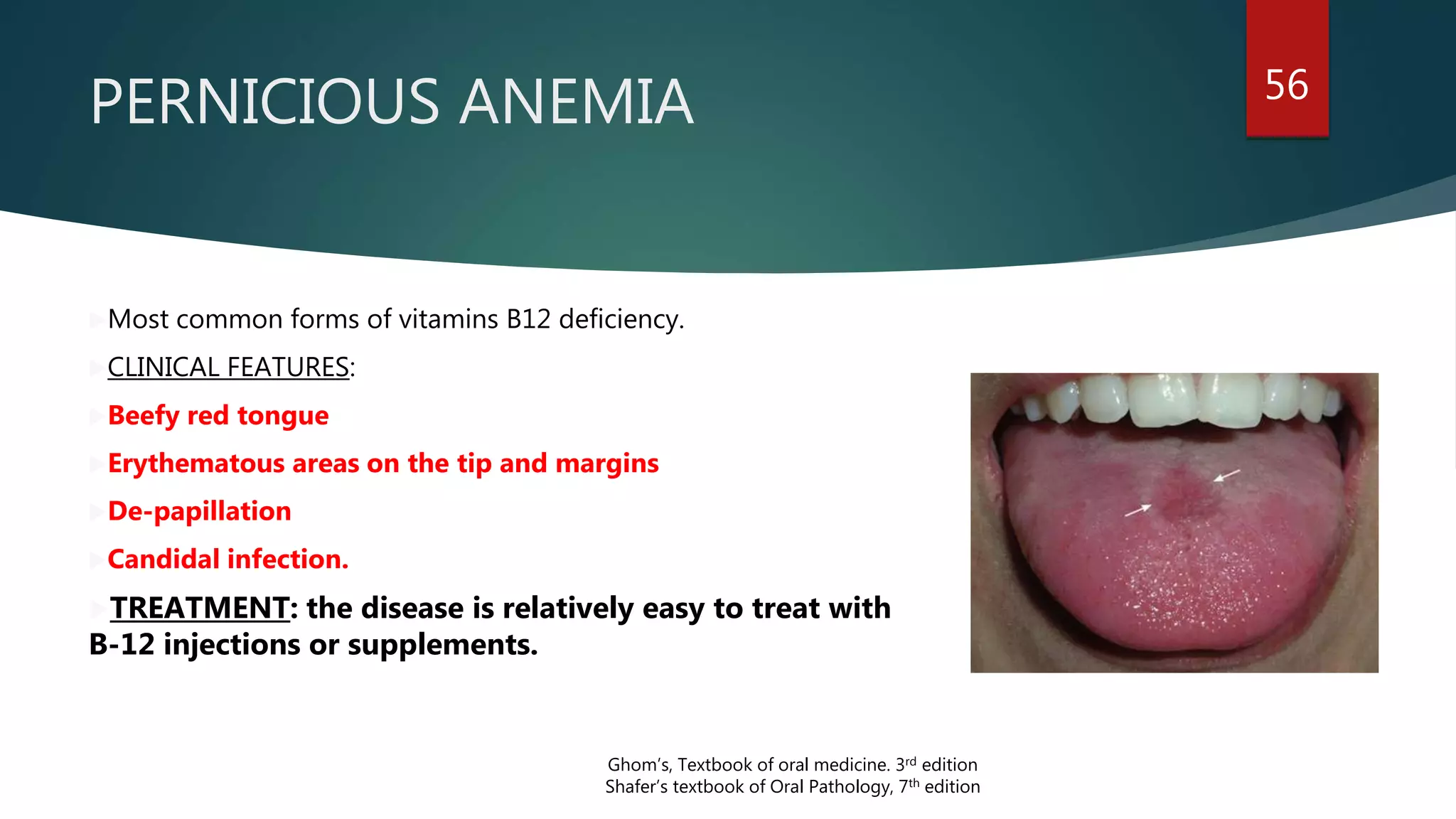
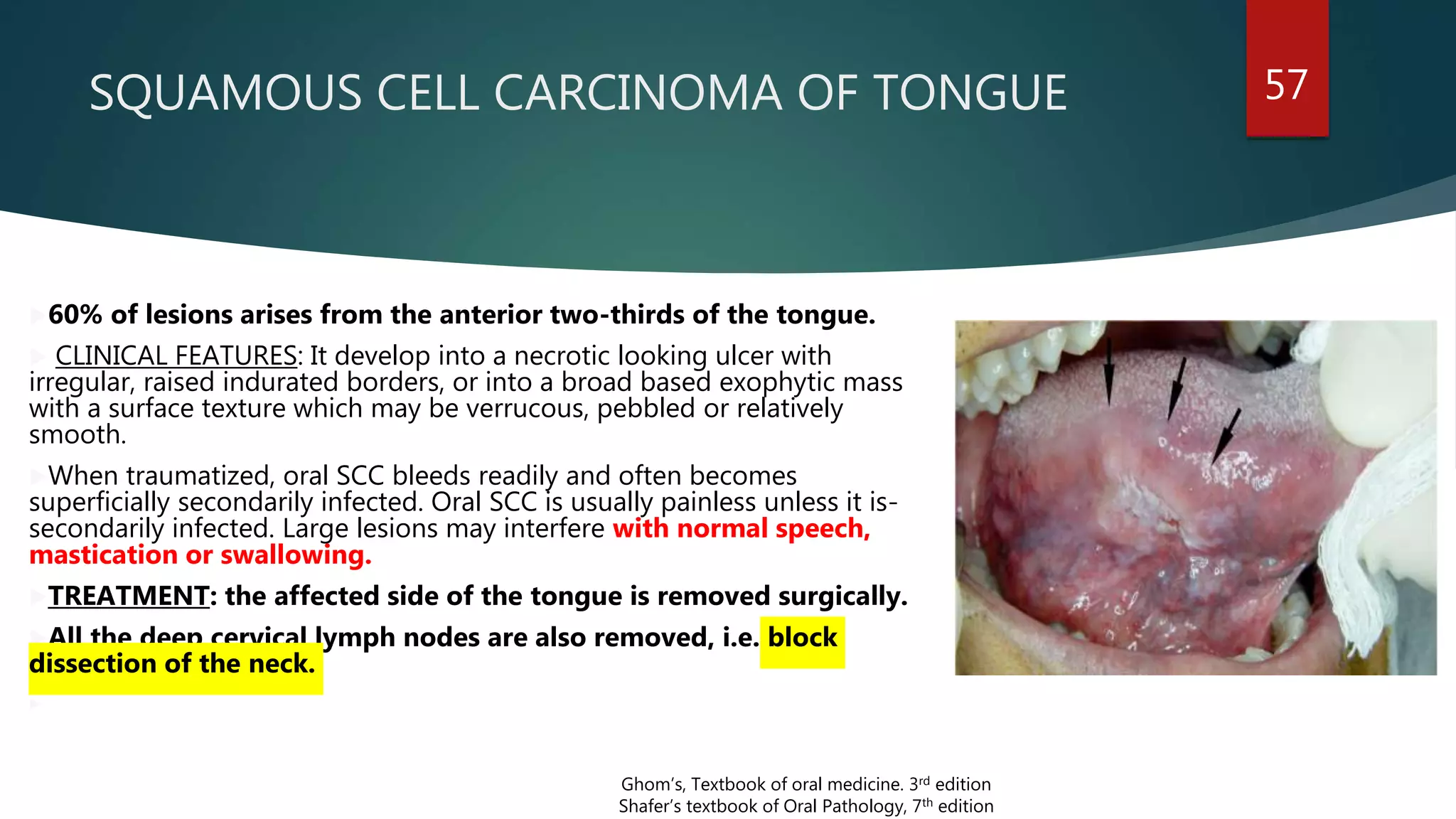
The document provides an overview of the anatomy of the tongue, including its parts, muscles, blood and nerve supply, development, and clinical applications. It discusses the root, tip, dorsum and inferior surface of the tongue. It describes the four types of papillae - vallate, fungiform, filiform and foliate. Both intrinsic and extrinsic muscles are defined. The arterial supply is from the lingual artery and venous drainage involves the deep lingual vein. Nerve supply includes the hypoglossal, lingual and glossopharyngeal nerves. Development occurs from the fusion of swellings from the pharyngeal arches. Anomalies and clinical features are also mentioned.