Preauricular incision is commonly used for TMJ surgeries. Other approaches include endaural, post-auricular, submandibular, post-ramal, hemicoronal, and coronal incisions. The choice depends on extent of pathology and surgeon preference.
APPROACHES
Ankylosis ingreek means stiff joint.
Ankylosis - as an abnormal immobility or consolidation of a joint due to
disease, injury or surgical procedure
TMJ ankylosis is a disabling condition - problems in mastication, digestion,
speech, function, cosmesis, and maintenance of oral hygiene.
Disturbances of facial growth and acute compromise of the airway, resulting in
physical and psychological disability
INTRODUCTION
6.
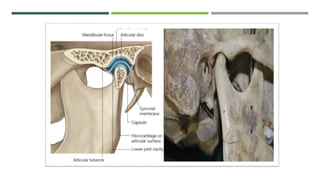
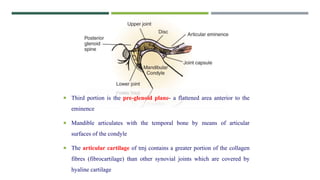
The articularportion of temporal bone is composed of three parts
The largest is articular or mandibular fossa- post slope of articular eminence
to post glenoid fossa- it is a ridge between fossa & external acoustic meatus
Second portion is the articular eminence- it is usually thick and serves as a
major component- of the TMJ- it serves as a attachment of collateral ligaments
7.
Third portionis the pre-glenoid plane- a flattened area anterior to the
eminence
Mandible articulates with the temporal bone by means of articular
surfaces of the condyle
The articular cartilage of tmj contains a greater portion of the collagen
fibres (fibrocartilage) than other synovial joints which are covered by
hyaline cartilage
9.
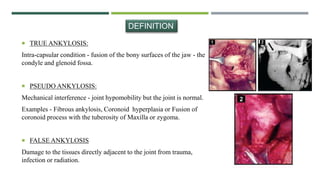
TRUE ANKYLOSIS:
Intra-capsularcondition - fusion of the bony surfaces of the jaw - the
condyle and glenoid fossa.
PSEUDO ANKYLOSIS:
Mechanical interference - joint hypomobility but the joint is normal.
Examples - Fibrous ankylosis, Coronoid hyperplasia or Fusion of
coronoid process with the tuberosity of Maxilla or zygoma.
FALSE ANKYLOSIS
Damage to the tissues directly adjacent to the joint from trauma,
infection or radiation.
DEFINITION
10.
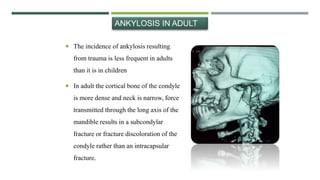
The incidenceof ankylosis resulting
from trauma is less frequent in adults
than it is in children
In adult the cortical bone of the condyle
is more dense and neck is narrow, force
transmitted through the long axis of the
mandible results in a subcondylar
fracture or fracture discoloration of the
condyle rather than an intracapsular
fracture.
ANKYLOSIS IN ADULT
11.
PATHOGENISIS
Trauma will bringabout extravasation of blood into
the joint space called haemarthrosis
Immobility of the joint is maintained over a prolonged
period , calcification and obliteration of a joint space
Many times initial fibrous bands lead toward
bony consolidation to ossification.
Activation of several molecular pathway, expression of
several genes including TGF and BMP.
12.
The disc undergoesprogressive destruction with flattening
of the glenoid fossa and the head of the condyle is
deformed and thickened.
INTRA ARTICULAR ANKYLOSIS
Resulting in narrowing or obliteration of the joint space
Bony fusion may extend well beyond the joint space to
involve the cranial base and even the sigmoid notch,
zygomatic arch, coronoid process.
In the severest form, it may include lateral pterygoid plate
and spine of sphenoid.
14.
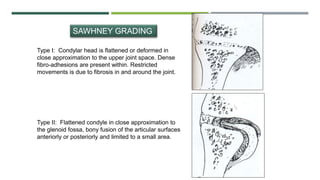
SAWHNEY GRADING
Type I:Condylar head is flattened or deformed in
close approximation to the upper joint space. Dense
fibro-adhesions are present within. Restricted
movements is due to fibrosis in and around the joint.
Type II: Flattened condyle in close approximation to
the glenoid fossa, bony fusion of the articular surfaces
anteriorly or posteriorly and limited to a small area.
15.
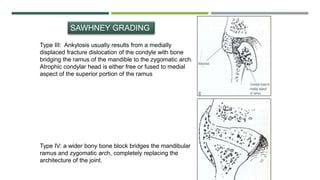
Type III: Ankylosisusually results from a medially
displaced fracture dislocation of the condyle with bone
bridging the ramus of the mandible to the zygomatic arch.
Atrophic condylar head is either free or fused to medial
aspect of the superior portion of the ramus
Type IV: a wider bony bone block bridges the mandibular
ramus and zygomatic arch, completely replacing the
architecture of the joint.
SAWHNEY GRADING
16.
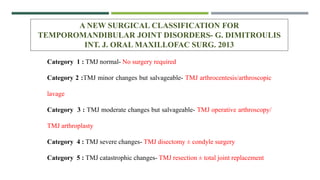
A NEW SURGICALCLASSIFICATION FOR
TEMPOROMANDIBULAR JOINT DISORDERS- G. DIMITROULIS
INT. J. ORAL MAXILLOFAC SURG. 2013
Category 1 : TMJ normal- No surgery required
Category 2 :TMJ minor changes but salvageable- TMJ arthrocentesis/arthroscopic
lavage
Category 3 : TMJ moderate changes but salvageable- TMJ operative arthroscopy/
TMJ arthroplasty
Category 4 : TMJ severe changes- TMJ disectomy ± condyle surgery
Category 5 : TMJ catastrophic changes- TMJ resection ± total joint replacement
17.
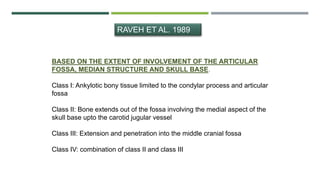
RAVEH ET AL.1989
BASED ON THE EXTENT OF INVOLVEMENT OF THE ARTICULAR
FOSSA, MEDIAN STRUCTURE AND SKULL BASE.
Class I: Ankylotic bony tissue limited to the condylar process and articular
fossa
Class II: Bone extends out of the fossa involving the medial aspect of the
skull base upto the carotid jugular vessel
Class III: Extension and penetration into the middle cranial fossa
Class IV: combination of class II and class III
18.
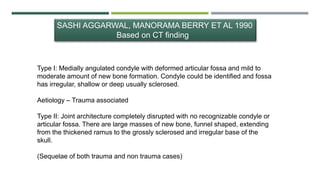
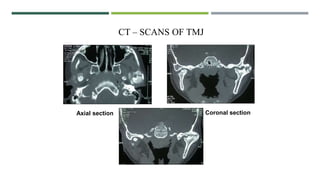
SASHI AGGARWAL, MANORAMABERRY ET AL 1990
Based on CT finding
Type I: Medially angulated condyle with deformed articular fossa and mild to
moderate amount of new bone formation. Condyle could be identified and fossa
has irregular, shallow or deep usually sclerosed.
Aetiology – Trauma associated
Type II: Joint architecture completely disrupted with no recognizable condyle or
articular fossa. There are large masses of new bone, funnel shaped, extending
from the thickened ramus to the grossly sclerosed and irregular base of the
skull.
(Sequelae of both trauma and non trauma cases)
19.
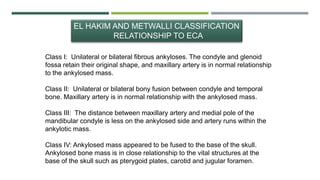
EL HAKIM ANDMETWALLI CLASSIFICATION
RELATIONSHIP TO ECA
Class I: Unilateral or bilateral fibrous ankyloses. The condyle and glenoid
fossa retain their original shape, and maxillary artery is in normal relationship
to the ankylosed mass.
Class II: Unilateral or bilateral bony fusion between condyle and temporal
bone. Maxillary artery is in normal relationship with the ankylosed mass.
Class III: The distance between maxillary artery and medial pole of the
mandibular condyle is less on the ankylosed side and artery runs within the
ankylotic mass.
Class IV: Ankylosed mass appeared to be fused to the base of the skull.
Ankylosed bone mass is in close relationship to the vital structures at the
base of the skull such as pterygoid plates, carotid and jugular foramen.
20.
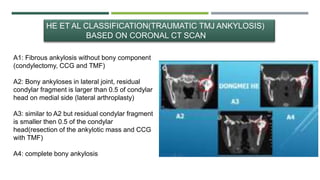
HE ET ALCLASSIFICATION(TRAUMATIC TMJ ANKYLOSIS)
BASED ON CORONAL CT SCAN
A1: Fibrous ankylosis without bony component
(condylectomy, CCG and TMF)
A2: Bony ankyloses in lateral joint, residual
condylar fragment is larger than 0.5 of condylar
head on medial side (lateral arthroplasty)
A3: similar to A2 but residual condylar fragment
is smaller then 0.5 of the condylar
head(resection of the ankylotic mass and CCG
with TMF)
A4: complete bony ankylosis
21.
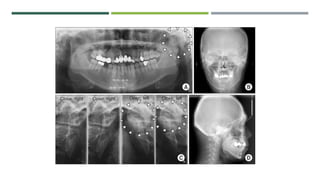
DIAGNOSIS
Diagnosis based onHistory, Clinical, Radiographic
examination.
Norman Rowe
1. H/O Injury or infection of the jaws.
2. Inability to open mouth or marked limitation.
3. Slight motion of the condyle of the non-involved side.
4. Slight motion from springing of the fibro-osseous tissue on the involved
side; in the bilateral case, movement may be impossible.
22.
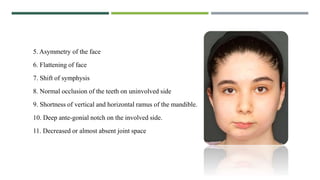
5. Asymmetry ofthe face
6. Flattening of face
7. Shift of symphysis
8. Normal occlusion of the teeth on uninvolved side
9. Shortness of vertical and horizontal ramus of the mandible.
10. Deep ante-gonial notch on the involved side.
11. Decreased or almost absent joint space
24.
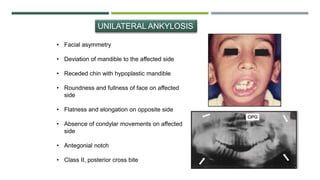
UNILATERAL ANKYLOSIS
• Facialasymmetry
• Deviation of mandible to the affected side
• Receded chin with hypoplastic mandible
• Roundness and fullness of face on affected
side
• Flatness and elongation on opposite side
• Absence of condylar movements on affected
side
• Antegonial notch
• Class II, posterior cross bite
25.
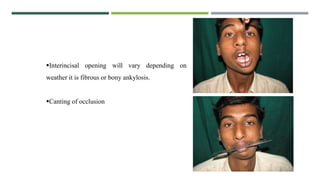
Interincisal opening willvary depending on
weather it is fibrous or bony ankylosis.
Canting of occlusion
26.
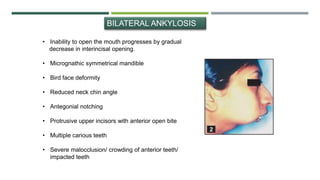
BILATERAL ANKYLOSIS
• Inabilityto open the mouth progresses by gradual
decrease in interincisal opening.
• Micrognathic symmetrical mandible
• Bird face deformity
• Reduced neck chin angle
• Antegonial notching
• Protrusive upper incisors with anterior open bite
• Multiple carious teeth
• Severe malocclusion/ crowding of anterior teeth/
impacted teeth
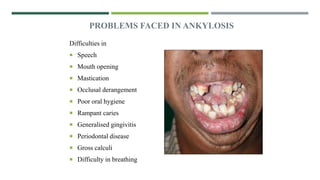
AIMS AND OBJECTIVESOF SURGERY
• Release of ankylosed mass and creation of a gap to mobilize the joint.
• Creation of a functional joint.
a. To improve patient’s nutrition.
b. To improve patient’s oral hygiene.
c. To carry out necessary dental treatment.
• To reconstruct the joint and restore the vertical height of the ramus.
• To prevent recurrence
• To restore normal facial growth pattern (based on functional matrix theory).
• To improve aesthetics and rehabilitate the patient (cosmetic surgery may be
carried out at a later date or at second phase).
35.
SURGICAL TREATMENT INCHILDREN
Two objectives
1. To improve mandibular function
2. Normal growth and development
1. Type 1&2 high condylar shave. 3-4mm of gap. Disc to be
mobilized
2. Destroyed condyle to be replaced by grafts
36.
SURGICAL TREATMENT INADULTS
Functional deficit - caused by hypomobility or
dentofacial deformity
Corrective orthognathic procedures after
correction of hypomobility.
37.
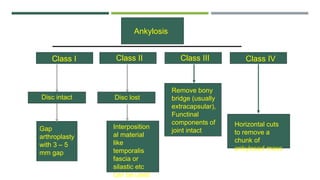
Ankylosis
Class I ClassII Class III Class IV
Disc lost
Disc intact
Gap
arthroplasty
with 3 – 5
mm gap
Interposition
al material
like
temporalis
fascia or
silastic etc
can be used
Remove bony
bridge (usually
extracapsular),
Functinal
components of
joint intact
Horizontal cuts
to remove a
chunk of
ankylosed mass
38.
J Oral MaxilllofacSurg.. 1990 Nov;48:1145-1151.1990
J Oral Maxillofac Surg.. 2009 Sep;67 1996-78 kaban, Bouchard and Troulis
1) Aggressive resection of the fibrous or bony mass
2) Coronoidectomy on affected side
3) Coronoidectomy on opposite side if steps 1 and 2 do not result in MO of 35 mm
4) Lining the joint with temporalis fascia or cartilage,
5) Reconstruction of the resected condyle unit with either DO or CCG and rigid
fixation
6) Early mobilization of the jaw, if DO then, mobilize on the day of surgery and if
CCG is used then early mobilization with minimal IMF( not more than 10 days)
7) Aggressive physiotherapy.
KABANS PROTOCOL- PERROT AND FISCHER
39.
• BRISMENT FORCE
•CONDYLECTOMY (FIRST PERFORMED BY HUMPERY IN1856)
• GAP ARTHROPLASTY (FIRST DOCUMENTED WAS BY ABBE)
• INTERPOSITIONALARTHROPLASTY
• RECONSTRUCTION OF JOINT
• COSMETIC REHABILITATION
DIFFERENT TREATMENT
METHODS
40.
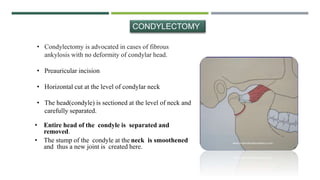
• Condylectomy isadvocated in cases of fibrous
ankylosis with no deformity of condylar head.
• Preauricular incision
• Horizontal cut at the level of condylar neck
• The head(condyle) is sectioned at the level of neck and
carefully separated.
CONDYLECTOMY
• Entire head of the condyle is separated and
removed.
• The stump of the condyle at the neck is smoothened
and thus a new joint is created here.
41.
• Loss ofvertical height of the ramus.
• In case of bilateral condylectomy, it may create an
anterior open bite.
• In unilateral cases, there may be deviation of the jaw
on opening.
COMPLICATION
42.
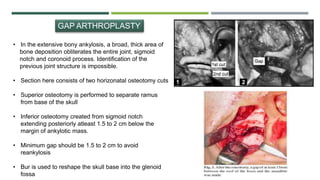
GAP ARTHROPLASTY
• Inthe extensive bony ankylosis, a broad, thick area of
bone deposition obliterates the entire joint, sigmoid
notch and coronoid process. Identification of the
previous joint structure is impossible.
• Section here consists of two horizonatal osteotomy cuts
• Superior osteotomy is performed to separate ramus
from base of the skull
• Inferior osteotomy created from sigmoid notch
extending posteriorly atleast 1.5 to 2 cm below the
margin of ankylotic mass.
• Minimum gap should be 1.5 to 2 cm to avoid
reankylosis
• Bur is used to reshape the skull base into the glenoid
fossa
43.
• Chances ofcreating excessive gap and reducing
vertical height of ramus.
• Anterior open bite due to excessive bone removal.
• Reankylosis due to bony contact between the cut ends.
COMPLICATION
44.
INTERPOSITIONAL ARTHROPLASTY
This isa modification of gap arthroplasty
Currently the protocol of choice
Materials are interposed in between the ramus of the mandible
and base of the skull to avoid re ankyloses.
The procedure involves creation of gap, barrier is inserted
between the two surfaces to avoid recurrence and to maintain
vertical height of the ramus.
45.
• Foreign bodyreaction with alloplastic materials
placed in surgical gap.
• Difficulty in suturing from the medial aspect.
• Complications associated with second surgical site
in case of autogenous graft.
COMPLICATION
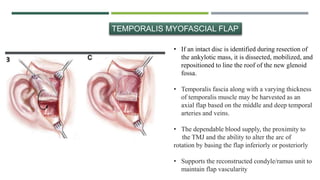
• If anintact disc is identified during resection of
the ankylotic mass, it is dissected, mobilized, and
repositioned to line the roof of the new glenoid
fossa.
• Temporalis fascia along with a varying thickness
of temporalis muscle may be harvested as an
axial flap based on the middle and deep temporal
arteries and veins.
• The dependable blood supply, the proximity to
the TMJ and the ability to alter the arc of
rotation by basing the flap inferiorly or posteriorly
• Supports the reconstructed condyle/ramus unit to
maintain flap vascularity
TEMPORALIS MYOFASCIAL FLAP
48.
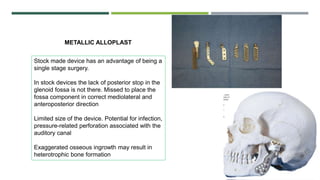
METALLIC ALLOPLAST
Stock madedevice has an advantage of being a
single stage surgery.
In stock devices the lack of posterior stop in the
glenoid fossa is not there. Missed to place the
fossa component in correct mediolateral and
anteroposterior direction
Limited size of the device. Potential for infection,
pressure-related perforation associated with the
auditory canal
Exaggerated osseous ingrowth may result in
heterotrophic bone formation
49.
Custom made devices- two stage surgery, two
CT scans.
Posterior stop available to prevent the
displacement of condyle posteriorly.
Custom made, modify the joint as per the
requirement.
Ductility, low coefficient of friction, high tensile
strength.
Expensive
NON METALLIC ALLOPLAST
51.
Pre auricularapproach
Modifications - Blair’s
- Thoma
- Al-Kayat and Bramley’s
- Popwich’s Modification of
Al-Kayat and Bramley’s
Endural approach
Post-auricular approach
Submandibular (Risdon’s) approach
Post ramal (Hind’s) approach
Hemicoronal approach
Coronal or Bicoronal approach
52.
Due to Anaesthesia
1.Difficulty in intubation
2. Aspiration of blood clot, as throat cannot be packed prior to
surgery.
3. Need expertise endotracheal intubator.
COMPLICATION
53.
Ankylosis presentsa formidable challenge to the oral and
maxillofacial surgeon.
Overall treatment is a long- term project that includes the
orthodontist , oral and maxillofacial surgeon, pediatric dentist ,
psychologist and physiotherapist as part of the health care team.
The patient’s post-operative commitment to physiotherapy and jaw-
stretching excercise determine the ultimate success.
CONCLUSION
54.
DURING SURGERY
1. Haemorhage
2.Damage to EAM
3. Damage to zygomatic and temporal branch of facial nerve.
4. Damage to glenoid fossa.
5. Damage to auriculotemporal nerve.
6. Damage to parotid gland.
7. Damage to teeth during opening of the jaws with jaw stretcher.
8. Complication due to costocondral graft.
55.
POST OPERATIVE COMPLICATIONS
1.Infection
2. Open bite
3. Recurrence of ankylosis
4. Erosion and heterotopic bone formation after alloplastic TMJ
reconstruction.
5. Fracture of costochondral graft.
6. Overgrowth of costochondral graft
7. Undergrowth of costochondral graft.
8. Facial nerve paralysis.
56.
RARE COMPLICATIONS
1. Permanentfacial paralysis.
2. Dislocation of contralateral TMJ.
3. Temporary paralysis of muscles of mastication.
4. Delayed infection of scar.
5. Frey’s syndrome.
57.
Oral andMaxillofacial Surgery : Fonseca
Peterson’s Principals of Oral and Maxillofacial Surgery
Oral and Maxillofacial Surgery: Neelima Anil Malik
Textbook of temporomandibular joint dosorders- okeson
8th edidtion.
REFERENCES