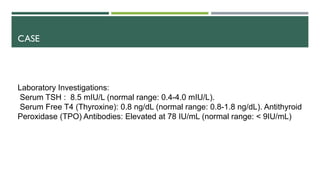
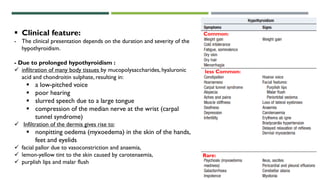
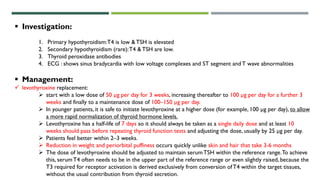
Khadeeja Nasser, a 35-year-old woman, presented with fatigue, weight gain, cold intolerance, dry skin, constipation, and irregular periods over the past six months. Examination found fatigue, puffy face, slow pulse, dry skin, and sluggish reflexes. Labs found elevated TSH and low T4, with positive thyroid peroxidase antibodies. This suggests Hashimoto's thyroiditis causing hypothyroidism. Hypothyroidism presents with the symptoms described and is diagnosed by elevated TSH and low T4. It is managed with levothyroxine replacement.