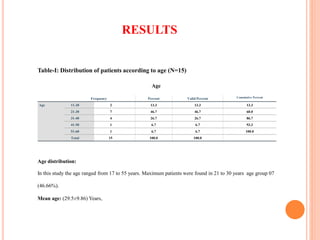
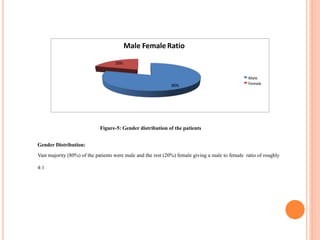
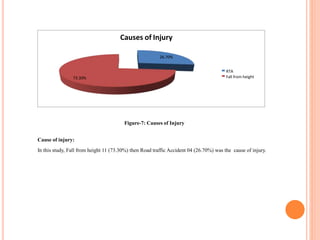
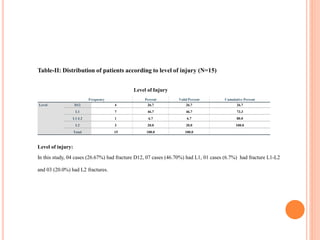
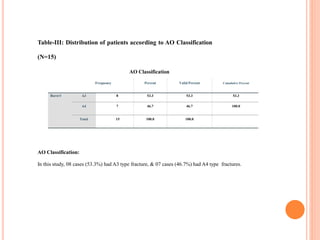
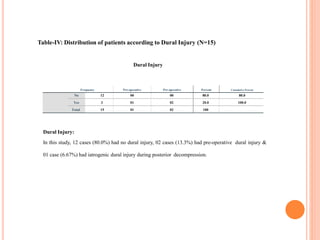
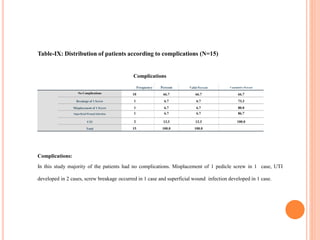
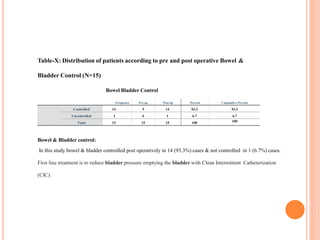
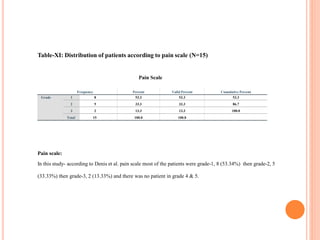
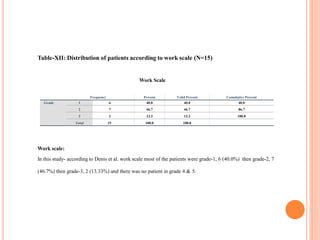
This study evaluated the functional outcomes of 15 patients who underwent thoracolumbar burst fracture stabilization using pedicle screw fixation and rods. Most patients were males between 21-30 years old, with falls being the primary cause of injury. The L1 vertebrae was most commonly fractured. Post-operatively, most patients experienced reduced pain and improved mobility, with 86.66% showing excellent or good functional outcomes and a mean hospital stay of 13 days. The results demonstrate pedicle screw fixation to be an effective procedure for stabilizing thoracolumbar burst fractures.










































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



