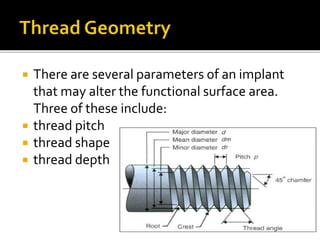
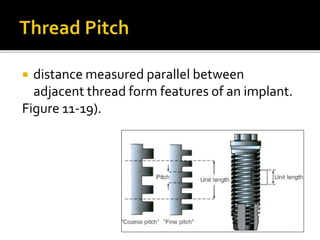
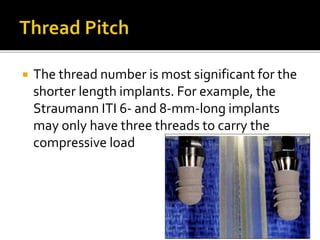
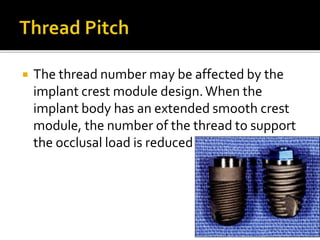
This document discusses various aspects of dental implant design that influence bone loading and integration. It describes different implant body designs (e.g. cylinder, tapered), surface conditions (e.g. machined, rough), and thread designs (e.g. V-thread, square thread). Specific design features like thread pitch, depth, and crest module dimensions also impact load transfer and stress distribution. The ideal implant design provides adequate surface area for initial stability and load transfer while minimizing shear forces on the bone.





















































![NEW dental implant design [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/newimplantdesignautosaved-250614065418-013f8c1f-thumbnail.jpg?width=640&height=640&fit=bounds)









![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















