Downloaded 167 times

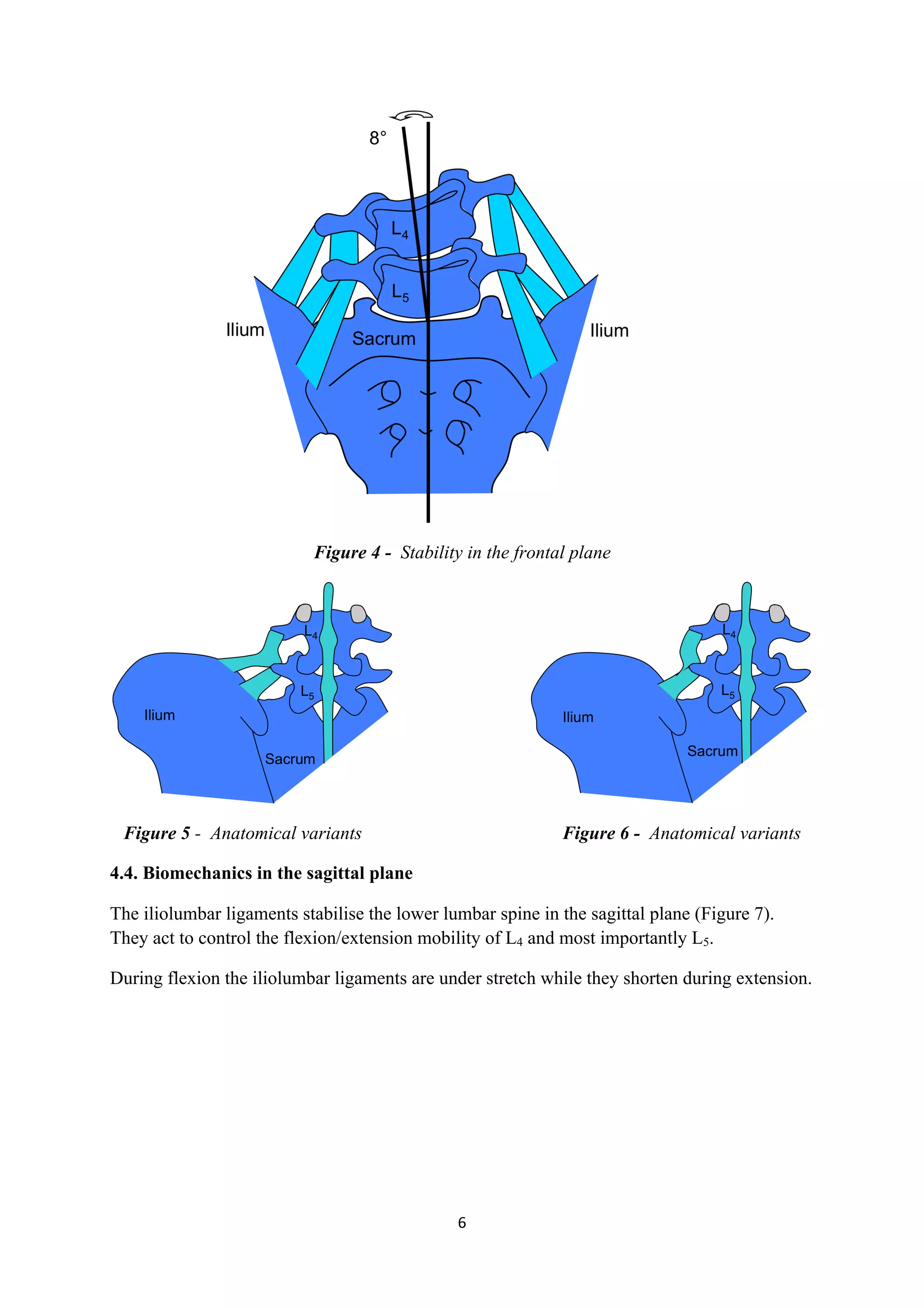
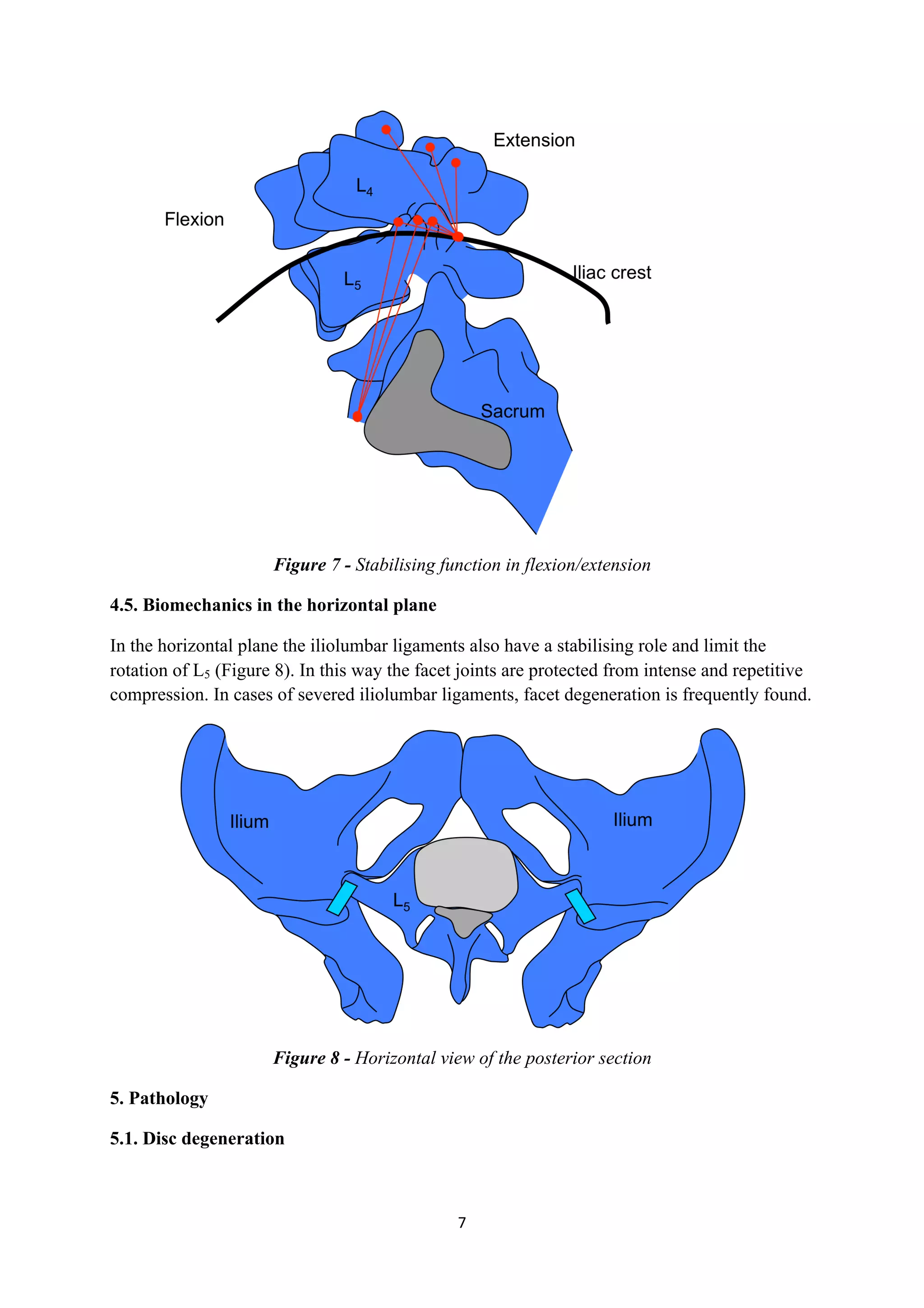

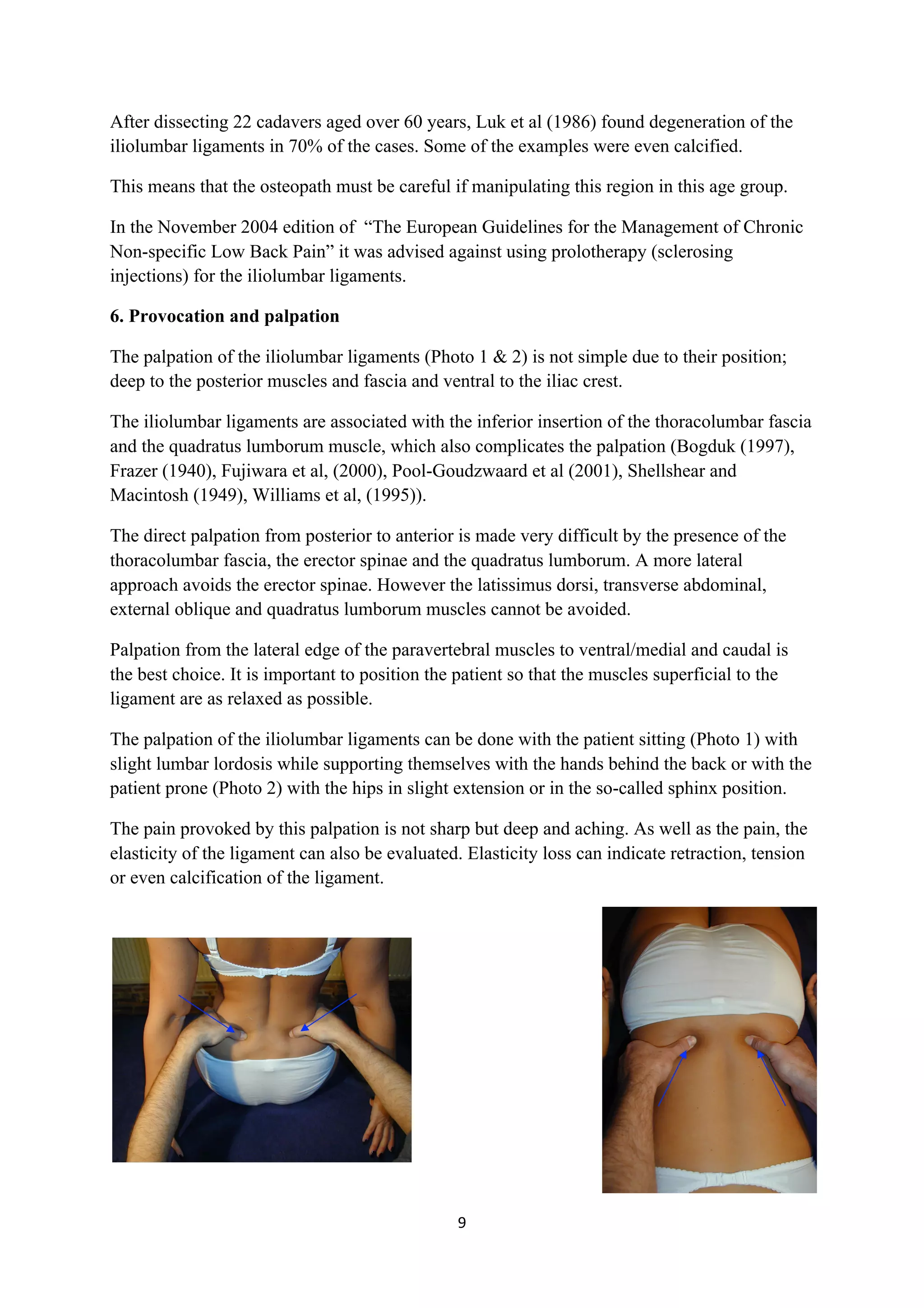
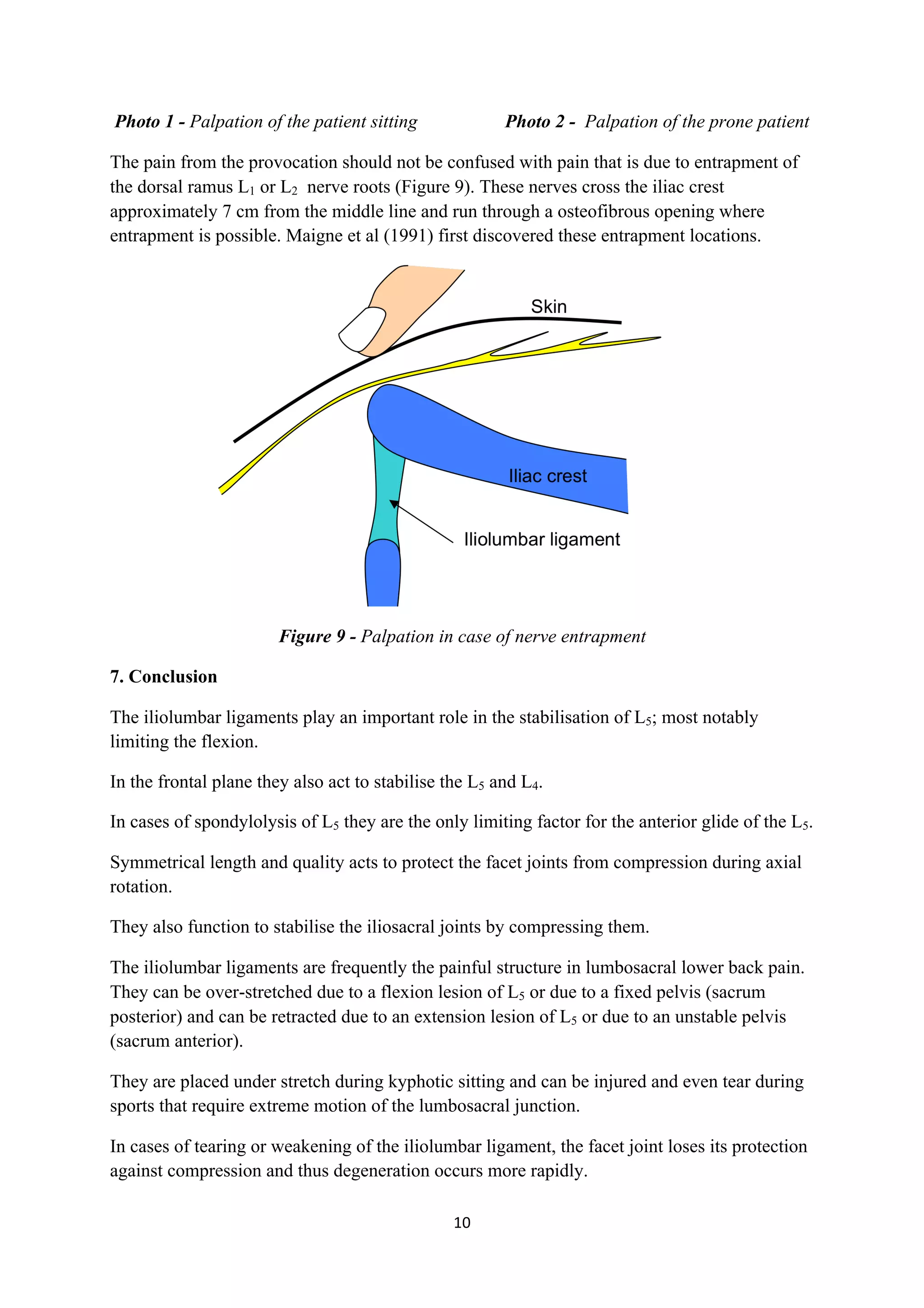

This document presents a comprehensive literature review on the iliolumbar ligaments, detailing their anatomical development, variations, and biomechanical functions in relation to spinal stability. It discusses the role of these ligaments in both healthy and pathological conditions, alongside findings from various anatomical studies and their implications for osteopathic practice. The document also highlights the challenges in palpating the iliolumbar ligaments due to their anatomic positioning and the surrounding musculature.




























































































