Download as PDF, PPTX
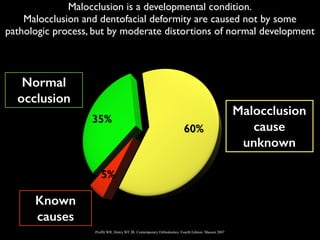
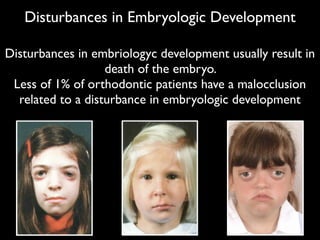
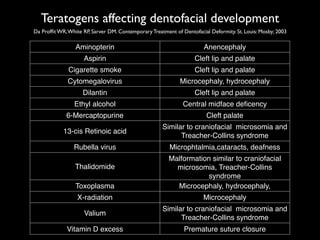
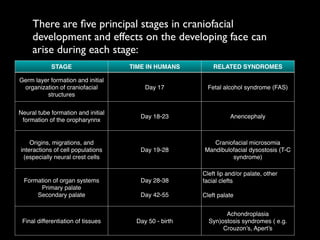
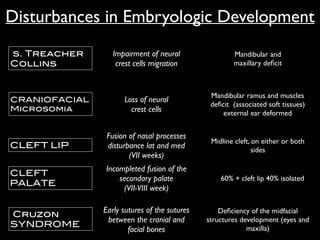
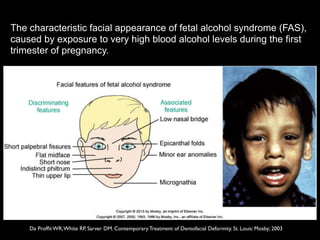
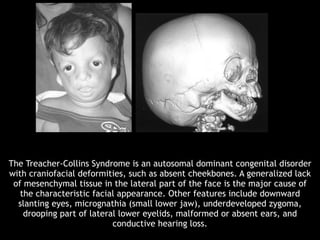

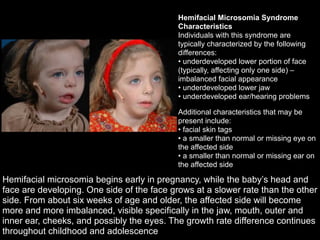
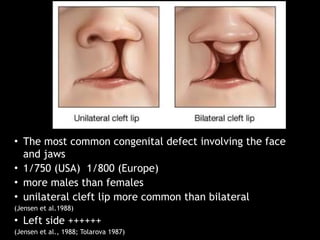
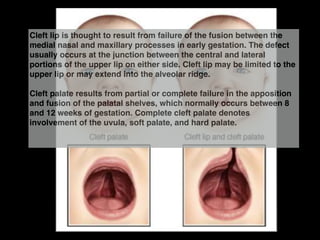
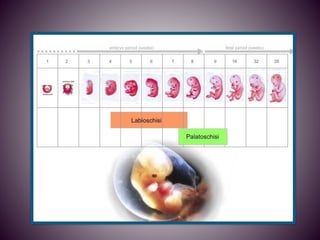
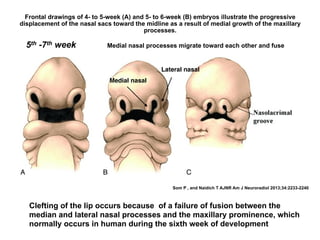
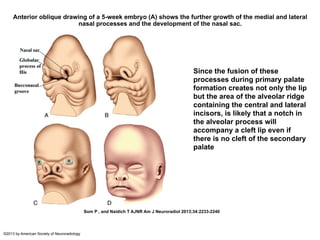

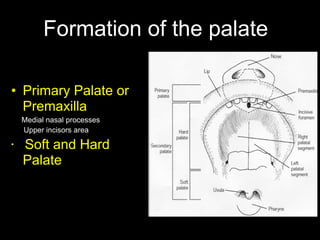
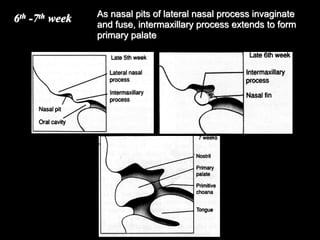
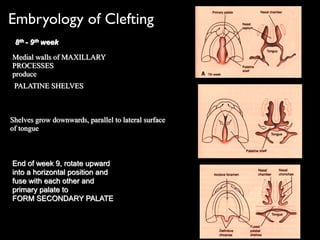
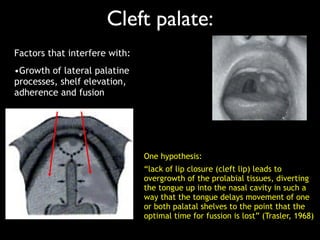
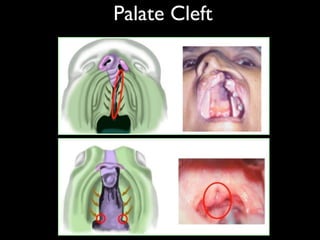
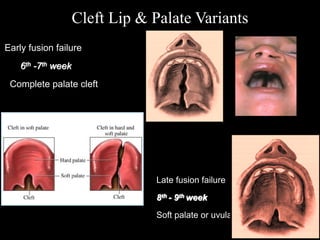
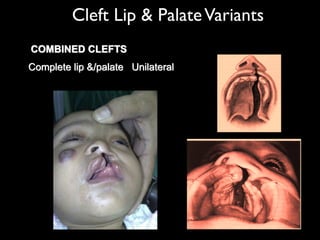
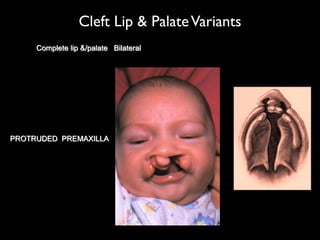
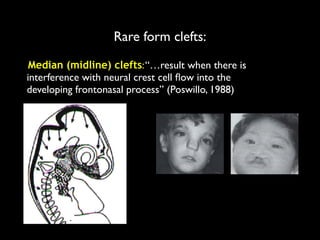
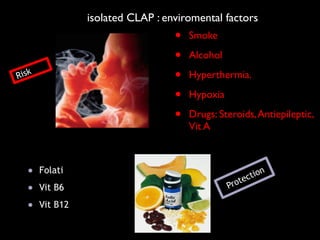

















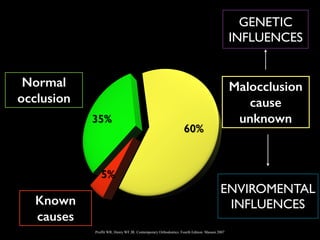
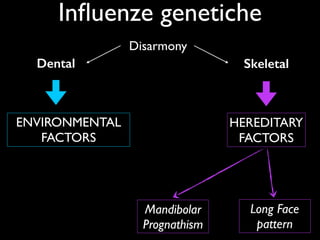
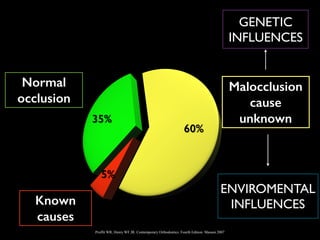










The document discusses the etiology of orthodontic problems, primarily malocclusion, which is attributed to a range of factors including genetic, environmental influences, and disturbances in embryonic development. It details various congenital conditions like cleft lip and palate, Treacher Collins syndrome, and hemifacial microsomia, outlining their developmental stages, genetic components, and clinical implications. The management of these conditions is highlighted as a multidisciplinary approach that integrates surgical, dental, psychological, and genetic considerations throughout the patient's development.










































































































