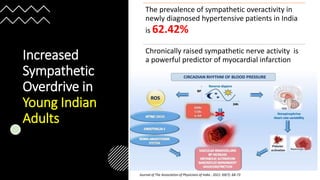
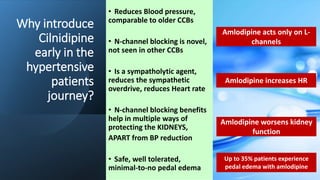
This patient is a 44-year-old male with uncontrolled hypertension for 5 years on Amlodipine and Ramipril. He has grade 1 retinopathy, elevated uric acid, mild microalbuminuria, and newly diagnosed diabetes. He complains of anxiety, difficulty sleeping, palpitations, and mild ankle edema.
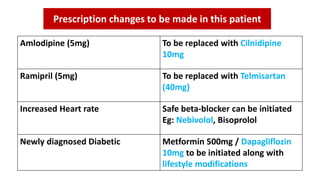
The next best steps are to change medications to better control his blood pressure and protect his organs. Cilnidipine should replace Amlodipine due to its additional sympatholytic and reno-protective effects. Telmisartan should replace Ramipril as it provides better blood pressure control throughout the day. A beta-blocker like Nebivolol can be


![Concerns in this case:
•Patient is: Uncontrolled Hypertensive (152/98 mmHg)
on ABPM despite being on 2 antihypertensives
[Lisinopril(5mg) and Amlodipine (5mg)]
•Grade 1 retinopathy – indicative of end-organ damage ,
also suggestive from eGFR and microalbuminuria
•Patient complains of: High HR, Anxiety, nervousness,
Palpitations – signs of sympathetic overdrive
•Elevated uric acid levels](https://image.slidesharecdn.com/cilnidipineinrenoprotection-230717052744-1e89d13e/85/Cilnidipine-in-Renoprotection-pptx-6-320.jpg)


































![Elevated BP (003) [Autosavedbbbbhh].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/elevatedbp003autosaved-250330085856-4eee68fa-thumbnail.jpg?width=640&height=640&fit=bounds)























































